6.5 Free Transverse Myocutaneous Gracilis Flap
The transverse myocutaneous gracilis (TMG) flap is a relatively new method in breast reconstruction. Although it was first described by Yousif in 1992 and was used for breast reconstruction in one case, the technique was subsequently forgotten to some extent. It was only with the advent of skin-sparing mastectomy that the main indication for this type of flap in reconstructive breast surgery emerged—to provide autologous filling tissue in the context of immediate reconstruction.
However, this also suggests the potential shortcoming associated with the procedure. Due to its relatively narrow skin island, the flap can only be used for secondary reconstruction after mastectomy in special cases.
A considerable advantage with the TMG flap is the inconspicuous donor-site scar, which is located in a natural crease in the groin. In addition, the invariable vascular anatomy makes the technical procedure for raising the flap easier (in contrast to perforator flap procedures). The donor site can be closed quickly and easily, and the operating time can be reduced by using two simultaneous surgical teams. As it is not necessary to change the patient’s position on the table, closure of the donor site and anastomosis of the flap can be carried out simultaneously.
The limited volume of the flap and the narrow skin island represent disadvantages which mean that the procedure is limited to special cases in secondary reconstruction. Appropriate patient selection is therefore of crucial importance for achieving good results with this type of flap.
Patient Selection
The ideal candidate for breast reconstruction with a TMG flap should be slim, with a small to moderate breast and a greater fat volume in the upper thigh than in the lower abdomen. Oncologically, a skin-sparing mastectomy with immediate reconstruction should be justifiable. If the patient has more excess tissue in the lower abdomen and would benefit from an abdominoplasty from the aesthetic point of view, then a TRAM/DIEP reconstruction procedure is preferable. However, if equal amounts of tissue are available in the abdomen and medial thigh, and if a large skin surface from the lower abdomen is not needed, but only a filling volume for reconstruction, then the TMG flap is a suitable reconstruction procedure ( Fig. 6.63 ). In rare situations in which the patient has large breasts and insufficient tissue in the lower abdomen and explicitly requests autologous reconstruction, two TMG flaps for reconstruction of a large breast can be considered. However, it should be noted that this represents an extremely demanding surgical procedure, and the higher micro-surgical risk due to the need for four microanastomoses and two independent recipient vessels has to be considered very carefully.
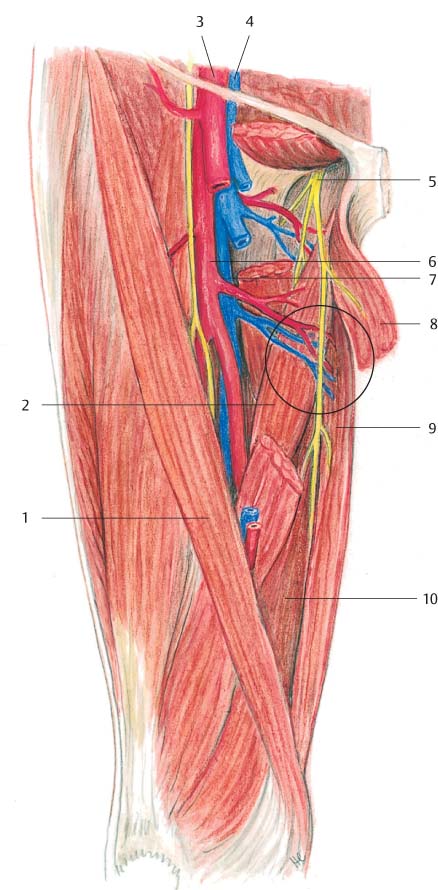
Anatomy of the TMG Flap
The gracilis muscle originates at the inferior pubic ramus and radiates with its typical round tendon into the common tendon of the pes anserinus, inserting along with the semitendinosus and sartorius muscles at the tibial tubercle ( Fig. 6.60 ). It is regarded as a type II muscle flap, with a single dominant proximal vascular pedicle and with one or two additional minor, more distally located pedicles. The main vessel (the terminal branch of the medial circumflex femoral artery, or a more distally coursing parallel vessel) arises from the deep femoral artery and vein. The origin of the flap artery can be located immediately lateral to the adductor longus muscle. After giving off several large branches into the adductor longus and smaller ones into the adductor magnus muscle, the artery enters the gracilis muscle approximately 8 cm inferior to the pubic tubercle. The nerve—the anterior branch of the obturator nerve—is located approximately 2 cm cranial from the point at which the vessel enters the muscle.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


