Abstract
Masseter hypertrophy can be successfully treated nonsurgically with neurotoxin. The condition can result in a square, boxy face in women, giving them a masculine appearance. Bruxism and clenching can result in masseter hypertrophy. Three injections into the central, inferior, and posterior portion of the muscle, where it is the thickest, can result in improvement in 2 weeks. Noting anatomic landmarks while planning the injections minimizes complications.
52 Neurotoxins: Masseter Hypertrophy
Key Points
Masseter hypertrophy can cause both functional impairment (i.e., bruxism and pain) and aesthetic dissatisfaction (i.e., wide, boxy contour of lower face).
Neurotoxin treatment can improve patient’s functionality and cosmesis, and offer an effective, alternative mode of management to surgical reduction for masseter hypertrophy.
Almost all non-East Asian patients present with masseter hypertrophy associated with bruxism, whereas hypertrophy in the East Asian population is almost universally benign.
Masseter hypertrophy can occur unilaterally as well as bilaterally.
52.1 Preoperative Steps
52.1.1 Analysis
To evaluate, inspect the lower face for a boxy or square-shaped appearance.
Palpate for masseter hypertrophy and rule out bony contours, overdeveloped parotid, and thick adipose tissue as the cause of the widened lower face.
Assess skin laxity, as injections in patients with poor skin tone may cause exacerbation of jowls for up to 2 months after treatment.
To assess muscle bulk, palpate the masseter during both relaxation and contraction.
Use standard frontal view photographs for preoperative and postoperative analysis, with optional lateral views to note muscle contraction changes.
52.2 Procedural Steps
See Video 52.1.
52.2.1 Anatomical Considerations
The masseter is a three-layer masticatory muscle arising from the zygomatic arch and inserting on the lateral ramus and angle of the mandible.
Branches of the masseteric nerve are most commonly found in the lower middle third of masseter muscle.
The facial vein usually runs anterior to the muscle, and the facial artery usually runs anterior to the facial vein.
The parotid duct usually runs superior to a line drawn between the earlobe and oral commissure.
The risorius muscle may partially cover the anterior masseter.
Safety zone (Fig. 52.1):
Superior border: Imaginary line drawn between earlobe and oral commissure.
Inferior border: Mandibular border.
Anterior border: 1 cm posterior to the anterior edge of the masseter muscle.
Posterior border: Posterior masseter muscle.
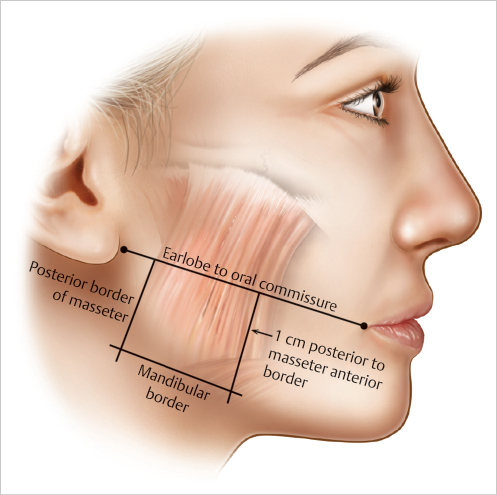
Fig. 52.1 Safety zone: Superior border: Earlobe to oral commissure. Posterior border: Posterior border of masseter. Anterior border: 1 cm posterior to masseter’s own anterior border. Inferior border: Mandibular border.
52.2.2 Injection Technique
Dosage of onabotulinum toxin A is divided equally among three injections per single masseter muscle.
Masseteric thickness determines the total dosage of onabotulinum toxin A per muscle:
Mild hypertrophy: 20 to 25 U
Moderate hypertrophy: 25 to 30 U
Severe hypertrophy: 30 to 40 U
Inject using a 30-gauge needle with a 1-mL syringe.
Injection sites:
Usually three injection sites per side (Fig. 52.2):
First injection: Thickest, central region of the muscle bulge, usually 1.5 cm superior to mandibular angle.
Second and 3rd injections: Distribute equidistant from the 1st across the bulging surface to form a triangle, staying inferior and posterior on the muscle to prevent inadvertent paralysis of the pterygoids and to prevent diffusion to the mimetic muscles.
For severe hypertrophy, total dosage may be divided into 4 + injection sites, distributed evenly to prevent post-treatment muscle bulging.
Technical tips:
To prevent inadvertent diffusion and paralysis of the medial and lateral pterygoids, stay below the sigmoid notch of the mandible.
Stay posterior on the muscle to avoid anterior diffusion of botulinum toxin into the risorius, the zygomaticus major and minor, and the levator anguli oris muscles to prevent facial expression and smile asymmetry.
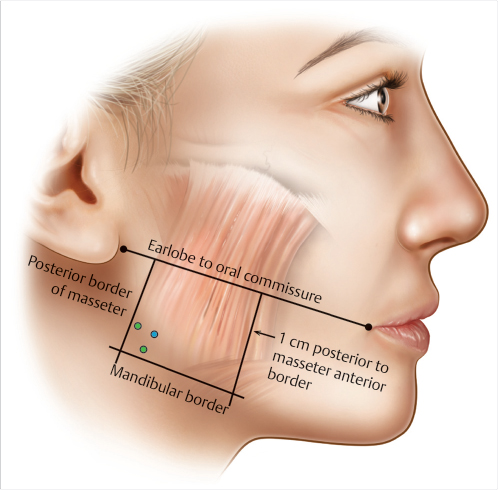
Fig. 52.2 Injection sites: 1st injection (blue) in thickest, central region of the muscle bulge, usually 1.5 cm superior to the mandibular border. Second and third injections (green) equidistant from the first site, evenly distributed over the bulge, staying inferior and posterior on the masseter.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


