Abstract
Microbotox is a technique where microdroplets of onabotulinumtoxinA are injected into the superficial layers of the skin and soft tissues of the face and neck as a superficial carpet of tiny drops to reduce fine lines and wrinkles, improve skin texture, and sheen and improve lower face and cervicomental contouring without compromising muscle function or mobility. Droplet size and not the dose is the most important consideration when injecting botulinum toxin into the face and neck.
Microdroplets have a limited diffusion capacity with the result that the injected onabotulinumtoxinA remains more targeted at the deep dermal level or where the superficial fibers of the facial muscles are inserted into the undersurface of the dermis. As a result, deeper muscular activity is retained and patients look and feel more natural.
Three mixtures of microbotox are employed: Microbotox-20 which contains 20 units of onabotulinumtoxinA in a 1-mL syringe of diluted toxin (used for pores and fine lines) over the infraorbital and central T-zone areas, Microbotox-24 which contains 24 units in 1 mL solution that includes lidocaine and is used for upper and lower face and neck in thin-skinned individuals such as females, and Microbotox-28 which contains 28 units in 1 mL solution and is used for upper and lower face and neck in those with thicker skin such as males. Effects last for 3 to 4 months.
50 Microbotox of the Face, Neck, and Scars
50.1 Underlying Principle and Concepts
With the advent of onabotulinum toxin and its popularization since the mid-1990s, on-label indications for the drug around the world include a five-point injection technique for the glabellar frown lines (20 units), a six-point injection technique for the crow’s feet (24 units), and a five-point technique for the forehead (20 units).
Each of these points is a droplet of 0.1 mL containing 4 units of standard onabotulinum toxin. A standard bottle of onabotulinum toxin is usually prepared with 2.5 mL of saline to make the calculation of dose administration easier to understand: 0.5 mL is 20 units, 0.6 mL is 24 units, and 0.7 mL is 28 units. A 1-mL syringe of standard onabotulinum toxin therefore contains 40 units.
Doctors have largely followed these on-label guidelines with the consequence that patients often return complaining that their forehead feels stiff, eyebrows are immovable and at a lower position than before injection, and they also notice deeper infraorbital and cheek creases appearing below the region of crow’s feet blockade, thereby conferring an unwanted, unnatural “Botoxed” appearance. In some cases, they may experience upper eyelid ptosis due to diffusion of the toxin into the levator muscles.
This author realized that too much toxin was being administered and that the most important consideration when injecting onabotulinum toxin was not the dose but the droplet volume. Large droplets of 0.1 or 0.05 mL have a much wider three-dimensional diffusion radius, which not only affects an area beyond the point of injection but also the entire depth of the soft tissue envelope.
Microbotox on the other hand uses microdroplets of 0.01 mL or less (Fig. 50.1).
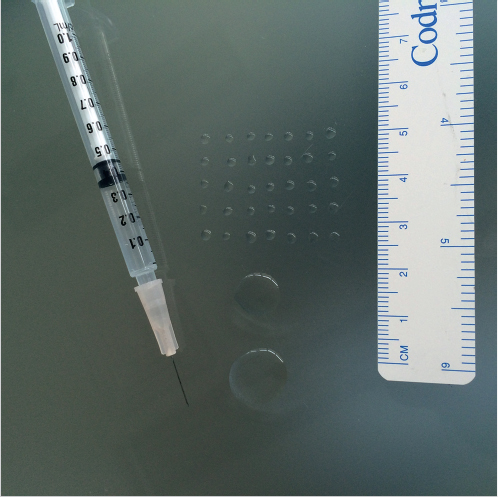
Fig. 50.1 Comparison between volume and size of a 0.1 or 0.05 cc droplet and a cluster of microbotox microdroplets all of which add up to 0.05 cc.
50.2 Microbotox of the Facial Upper Third
There are some patients who request and like a totally smooth and immovable forehead without a trace of movement in the glabella region and certainly no crow’s feet lines. Standard doses of Botox can achieve this.
For those patients who want a more natural or refined appearance, with some movement of all the muscles, the microbotox technique is extremely useful as this does not paralyze the muscles completely (Fig. 50.2a, b).
A third category is those patients who may need some standard macrodroplets into specific muscles such as the medial glabellar frown (corrugator origin) or the central crow’s feet region just lateral to the lateral canthus but a microbotox technique to the forehead. Here, the author uses both standard as well as microbotox techniques in combination.
Each patient has to be individually assessed as different patterns of eyebrow elevation exist. Some patients are central “pullers” where the medial eyebrow is more elevated than the lateral aspect, some are lateral “pullers” where the eyebrow has a greater lateral elevation than medially and some are uniform “pullers” where the eyebrow elevates without any distortion in its shape. Microbototox-24 is used for females whilst Microbotox-28 is used in males with thicker skin and more active glabellar muscles.
As aesthetic trends have changed through the years and the emphasis is now on a more natural appearance, this author prefers to employ microbotox droplets for the entire facial upper third. There are much fewer complications and fewer complaints. Patients are informed that the effect will last from 3 to 4 months.
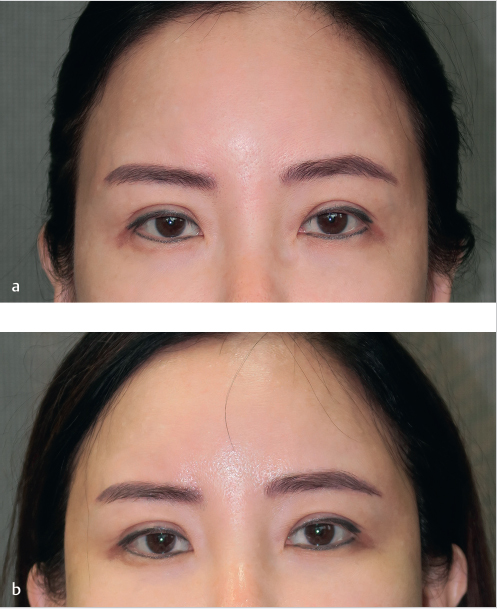
Fig. 50.2 (a, b) Microbotox of the upper facial third (forehead, glabellar, crow’s feet areas) showing a bright, lifted appearance of the eyebrows, smoothening of frown lines and improved skin appearance and reflectance.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


