Abstract
A defined jawline gives strength, character, and beauty to the face. The jawline elegantly enhances the face and gives a distinctive border between the face and neck. Nonsurgical interventions with injectable fillers such as hyaluronic acid (HA) fillers and non-HA fillers are an excellent tool for beauty enhancement and rejuvenation of lower face aging changes. The use of fillers to improve mandible projection and reduce jowl heaviness has become more popular as more people are seeking the means to combat signs of facial aging.
Fat atrophy, dermal collagen breakdown, subcutaneous volume loss, and bone resorption are the culprits that change the lower face. HA-based fillers are beneficial for jawline augmentation, as they have a medium to high G-primes and are used to reverse blunting of the angle of the mandible and lower face jowling. Non-HA fillers such as calcium-based fillers are useful to achieve more pronounced projection and support of bone resorption changes around the mandibular ligaments. Nonhyaluronic fillers have among the highest G-primes and act as biostimulators. Because of their unique biostimulatory properties and chemical composition, non-HA fillers cannot be dissolved and demand experienced injectors with comprehensive anatomical knowledge.
A stepwise approach to jawline contouring gives the best results. The areas which give the most effective jawline sculpting include four primary injection sites: the mandibular angle, the antegonial notch, the prejowl sulcus, and the junction of the anterior end of the mandibular body with the mentum. The volumizing lift of high-density fillers in these locations improves herniation of fat around the mandibular ligaments.
The ability of injectable fillers to alleviate subcutaneous volume loss and reduce tissue laxity has revolutionized medical aesthetics. Lower face and jawline fillers are minimally invasive procedures that reliably improve the jawline with excellent safety and efficacy.
44 Jaw Fillers
Key Points
Treatment of facial aging changes must address the maintenance of youthful jawline projection and correction of its volume changes. Jawline aging changes include skin with dermal collagen breakdown, fat pads with subcutaneous fat atrophy, and bone resorption.
Hyaluronic gel fillers and nonhyaluronic acid (non-HA) biostimulator injections are highly effective for correcting jawline aging changes. HA-based fillers are beneficial for moderate soft tissue augmentation, as they have a moderate to high G-prime, indicating the filler’s elastic ability to resist compression and improve volumization. Non-HA-based fillers help to achieve more robust augmented facial features because of their higher G-primes, ability to contour bone density changes, and ability to act as biostimulators to induce secondary neocollagenesis.
44.1 Preoperative Steps
44.1.1 Background Knowledge
Mandibular bone resorption is most prominent in locations with muscle attachments and vascular structure crossings, requiring correction. Changes in bone density contribute to jowling by causing bone to remodel in a convex configuration, causing retraction of the facial ligaments and muscles.
Assessment of the aging changes of the mandible should involve inspection of the retaining ligaments, the bony mandible, the prejowl sulcus, the masseter muscle, and the skin changes.
There are two key retaining ligaments within the jowl: the platysma mandibular ligament and the mandibular osseocutaneous ligament. Both of these ligaments work together to maintain tissue and muscle stability in the lower face. Filler injections supporting these ligaments will treat bone resorption changes by helping facial ligaments retain their mechanical effect on surrounding tissues. Myomodulation of lower face muscles by accurate filler placement around the mandibular ligaments also contributes to their improved function and lift.
Fillers can alleviate the appearance of jowls by improving bone projection of the mandible and maxilla, allowing for increased support of the drooping tissues in the prejowl area of the mandible and the mentum.
44.1.2 Preoperative Clinical Understanding
Patients should be counseled at least 7 days prior to injection to avoid any agents that could cause blood thinning such as aspirin, ibuprofen, Motrin (or any other nonsteroidal anti-inflammatory drugs [NSAIDs]), fish oils, or vitamin E. Alcohol consumption 7 days before and after injection is not advised, as this increases the risk of bruising and swelling.
44.1.3 Day of Procedure
Conduct a detailed health history assessment on patient’s known allergies, medical conditions or contraindications to potential fillers, prior filler, facial surgery, trauma, and implant history.
Makeup should be removed, and the face should be cleansed with 70% alcohol, chlorhexidine, or betadine to ensure sterile conditions.
Pretreatment pictures for photographic documentation should be taken for pre- and postprocedural comparisons.
44.1.4 Filler Selection
Patients exhibiting heavy jowling benefit most from high G-prime products such as calcium hydroxyapatite and high G-prime hyaluronic gel fillers. These dense fillers have viscoelastic properties that can mimic the support and contours of periosteum. Patients with superficial subcutaneous dermal thinning will benefit most from medium hyaluronic gel fillers, as their G-prime properties allow for plumping and hydration of dermal thinning.
Patients who are new to injectables, indecisive, or nervous about filler reversibility should be treated with hyaluronic fillers. Those with facial scar tissue changes who may have abnormal lymphatic and vascular supply after surgical procedures are also advised to use hyaluronic gel fillers. The effects of HA gel fillers can be reversed and dissolved with hyaluronidase (unlike non-HA fillers). Both HA fillers and non-HA fillers have a 12- to 24-month duration.
The sculpted and contoured aesthetic that often appeals to younger patients can be best achieved through non-HA fillers such as calcium hydroxyapatite. This is an implant composed of carboxymethylcellulose and calcium hydroxyapatite. Additionally, it is a biostimulator that can induce primary and secondary neocollagenesis wherever it is placed. Through neocollagenesis, the effects of these fillers continue post injection, and is unable to be reversed or dissolved.
Patients who are highly sensitive or have proven to be allergic or reactive to other injectables should consider non-HA calcium hydroxyapatite over HA, as it is biocompatible with human tissues and is nonantigenic. It is advisable that novice injectors start with HA fillers because of their reversibility and shorter duration.
44.1.5 Anatomy Assessment and Markings
Evaluate the medial and lateral malar fat pads for any deflation or descent, as it is important to determine if drooping and the weight of the cheek are contributing to jowling and jawline changes. It is important to revolumize the lateral maxillae and maxillary eminence.
Assess the ideal mandible angle (Fig. 44.1). This gonial angle is formed by the junction at the midpoint of the posterior border of the ramus and the inferior border of the body of the mandible (Fig. 44.1 and Fig. 44.2). This varies between gender, but a good standard for women to adhere to is 120 to 125 degrees and 130 to 140 degrees for men.
Evaluate the deep lateral chin compartment (Fig. 44.3). As described by Lamb and Surek in their textbook, Facial Volumization: An Anatomic Approach, this region contains a fat pad that is integral for providing volume to the prejowl sulcus. The fat pad can be located deep to the depressor anguli oris (DAO) muscle. This fat layer protects the mental nerve and because it is located close to the inferior labial artery, injecting filler into here requires caution.
Evaluate muscles that also influence jawline contours, such as the masseter muscle, which can make the jawline appear bulky. In addition to this, the DAO muscle contributes to the downwards pull around the mouth and the deep groove of the prejowl sulcus (Fig. 44.4). The DAO contributes to fat tissue descent in the prejowl sulcus region, the region directly inferior to the commissure and is in association with the mandibular ligament. The mandibular ligament suspends the sagging tissue that contributes to jowling from behind the marionette furrow and with filler correction, tissue suspension will be enhanced.
The masseter muscle is a two-layer structure, with a superficial and deep component located at the lateral surface of the ramus and mandibular angle (Fig. 44.5). Injections into the masseter muscle will cause the appearance of hypertrophic masseter muscles and must be avoided. Palpating the anterior border of the masseter muscle leads to the antegonial notch. It is important to know that the presence of a large mandibular antegonial notch is indicative of mandibular resorption changes, which should be addressed with filler to correct the contour deformity. From a point anterior to the prejowl sulcus, a cannula can be used with retrograde threading technique to place a high density, integrated hyaluronic filler.
At the junction of the anterior end of the mandibular body and mentum, linear retrograde threads of filler can be placed in several directions to support the oral commissure and lip and to extend contouring to the chin and mental crease. This increases maximum mandibular projection.
Placement of fillers surrounding the supportive mandibular ligaments is critical to alleviate the herniation of fat that creates jowls (Fig. 44.6). As described by Lamb and Surek in their textbook Facial Volumization: An Anatomic Approach, the platysma mandibular ligament can be found roughly 5 cm distal to the gonial angle, superior to the mandibular border. Injections here are beneficial, as this is a point of muscular stability for the platysma. The mandibular osseocutaneous ligament can be found by palpating between the anterior jowl and marionette line. It is located approximately 1 cm superior to the mandibular border and 5.5 cm from the gonial angle. Injections here will provide structural support and lift to sagging tissue, to create a youthful jawline.
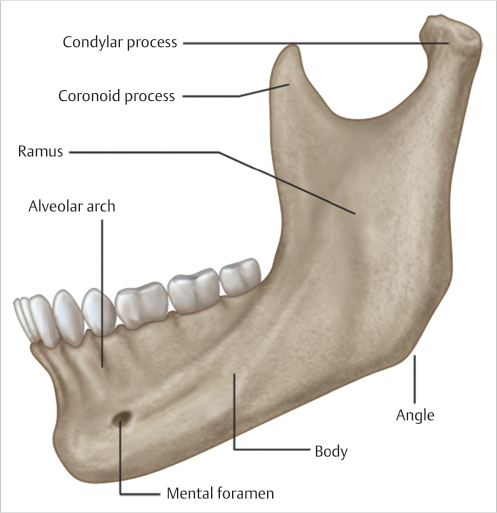
Fig. 44.1 Side-view depiction of the three-dimensional structure of mandible, the angle of the mandible, and the ramus of mandible. (Reproduced with permission from Watanabe K, Shoja MM. Anatomy for Plastic Surgery of the Face, Head, and Neck. Thieme; 2016.) 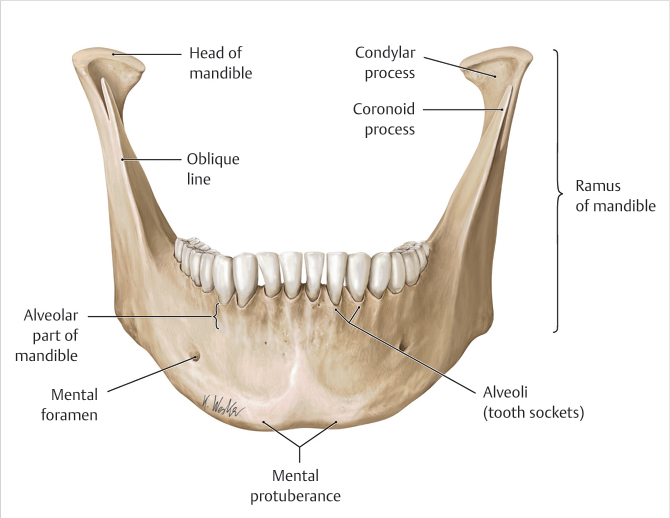
Fig. 44.2 Front-view depiction of the three-dimensional structure of mandible, the angle of the mandible, and the ramus of mandible. (Reproduced with permission from Watanabe K, Shoja MM. Anatomy for Plastic Surgery of the Face, Head, and Neck. Thieme; 2016.) 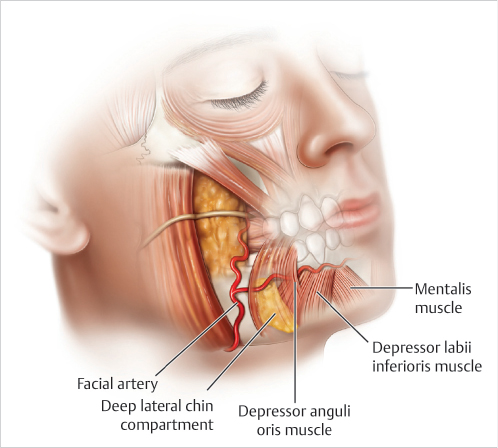
Fig. 44.3 Deep lateral chin compartment and inferior labial artery anatomical locations. 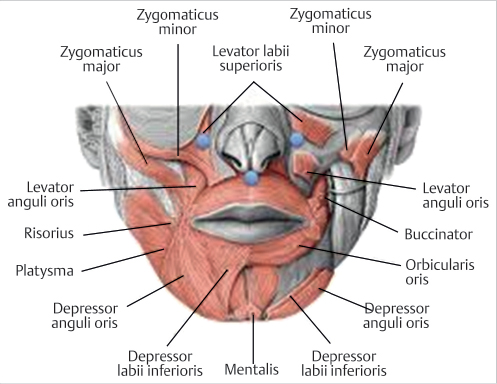
Fig. 44.4 Depressor anguli oris muscle location and structure. (Reproduced with permission from Benson BE, Blitzer A. Botulinum Neurotoxin for Head and Neck Disorders. Thieme; 2012.) 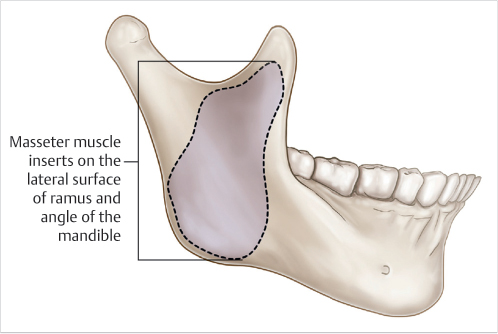
Fig. 44.5 Masseter anatomy. 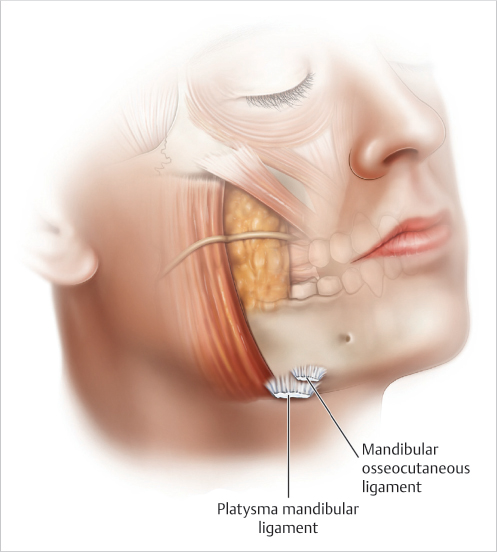
Fig. 44.6 Retaining ligaments within the jaw.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


