43 Costal Cartilage Harvest and Preparation for Rhinoplasty
Introduction
Costal cartilage is a valuable source of grafting material for nasal reconstruction, especially in the setting of extensive structural nasal defects or revision rhinoplasty. Although there are numerous approaches for harvesting costal cartilage, all methods rely on similar basic principles. An understanding of chest wall anatomy is important for obtaining costal cartilage with minimal donor site morbidity and complication. Carving the harvested cartilage into the appropriate shape with minimal postoperative warping requires further knowledge of the biomechanical properties of this unique reservoir. The aim of this chapter is to describe the role of costal cartilage for rhinoplasty, as well as provide the rationale and techniques for harvesting and carving grafts from this source.
Overview of Cartilage Sources: Advantages, Limitations, and Morbidity
Autologous materials include grafts directly harvested from the patient and are thus ideal due to their biocompatibility. 1 Nasal septal cartilage is the preference for rhinoplasty because it does not require a distinct field for harvest, is flat, and maintains its shape well. However, this source of cartilage is limited and can be insufficient, especially in revision operations. An additional source of cartilage is the concha of the ear. Although the donor site morbidity is minimal and the associated defect and scar is typically inconspicuous, the disadvantages include its relatively weak and curved structure that is not well suited for the majority of rhinoplasty grafts. Compared to the aforementioned graft sources, costal cartilage is a valuable option due to its relatively abundant supply. However, harvesting costal cartilage is associated with donor site morbidity such as pain, cosmetic deformity, chest wall clicking, and pneumothorax. Furthermore, carving costal cartilage into appropriately shaped grafts is encumbered with the concern of postoperative warping.
Indications and Uses
Costal cartilage is a highly beneficial graft source for rhinoplasty when septal and auricular cartilages are insufficient. This includes circumstances when the septal and auricular cartilage reservoirs are exhausted from prior surgery, the nasal defect is extensive, or the auricular cartilage is of inadequate strength to support the required grafting. Costal cartilage is strong, yet appropriately flexible, and is well suited for numerous graft types. 2 The costal cartilage grafts can be carved for structural support, such as for the caudal septum and the lateral nasal walls. The cartilage can also be fashioned as onlay grafts or diced cartilage grafts for cosmetic augmentation of the nasal dorsum. Smaller cartilage pieces can be carved into shield, cap, and rim grafts for further enhancing aesthetics.
Costal cartilage has most commonly been used for dorsal augmentation. For instance, the Asian nose typically has a flat dorsum and benefits from placement of a canoe-shaped dorsal onlay graft. 3 Augmentation techniques are also frequently utilized for many patients of Latin American 4 and African 5 , 6 descent. Revision rhinoplasty cases may require dorsal grafts due to prior overresection or to replace an alloplastic graft that has extruded or has become infected. Trauma may also produce a depressed dorsum requiring reconstruction of the nasal dorsum. This may be due to immediate collapse of the dorsum from the impact or indirectly as the result of saddling due to an untreated septal hematoma that has led to compromise of the nasal framework.
The versatility of costal cartilage enables a unique graft source for reconstructing numerous nasal deformities. In total nasal reconstruction, costal cartilage can be used to reconstruct the entire nasal framework. This cartilage source excels as a loadbearing structural unit, such as a columellar strut. The strength of these struts has been proven by effectively counteracting the collapsing forces of the deficient columella in cleft lip. 7
Anatomy
The costal cartilages are extensions of hyaline cartilage from the anterior ends of the ribs and contribute to the elasticity of the thoracic wall ( Fig. 43.1 ). Each of the 12 paired ribs articulate posteriorly with the respective thoracic vertebrae. Anteriorly, the first seven pairs of ribs, also known as true ribs, attach directly to the sternum through their respective costal cartilages. Typically the costal cartilages of ribs six and seven have an intercostal attachment. The remaining five pairs of ribs (8 through 12) either have an indirect attachment or no attachment to the sternum, and are known as the false ribs. 8 , 9 , 10
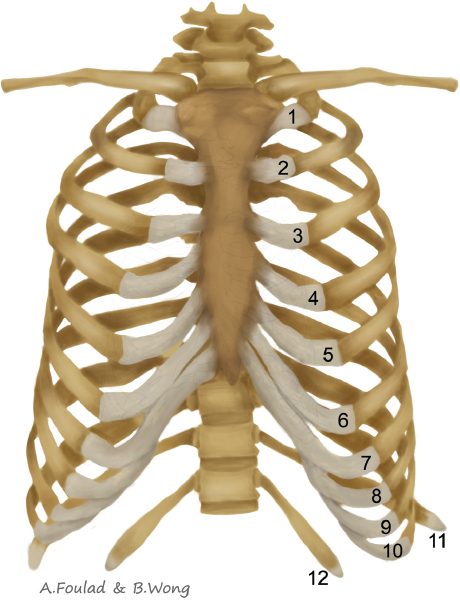
Conventionally, the costal cartilages of ribs 8, 9, and 10 are described as being attached to the costal cartilages of ribs 7, 8, and 9, respectively. Ribs 11 and 12 are often considered floating ribs because the costal cartilages of these ribs do not attach to the sternum or other ribs. However, from a surgical perspective, ribs 9 and 10 have also been described as floating ribs with no significant attachments to the costal margin. 8 , 11
There are a total of 11 intercostal spaces that contain three main groups of muscles. These intercostal muscles facilitate respiration and include, from superficial to deep, the external intercostal muscles, internal intercostal muscles, and innermost intercostal muscles. An intercostal neurovascular bundle runs along the inferior border of each rib and is located between the internal intercostal muscle and innermost intercostal muscle. The neurovascular bundle, arranged from superior to inferior, consists of a vein, artery, and nerve. Although the neurovascular bundle is conventionally described as running along the subcostal groove, there is evidence that there can be significant deviation, both more superior and inferior, from this expected route. 12
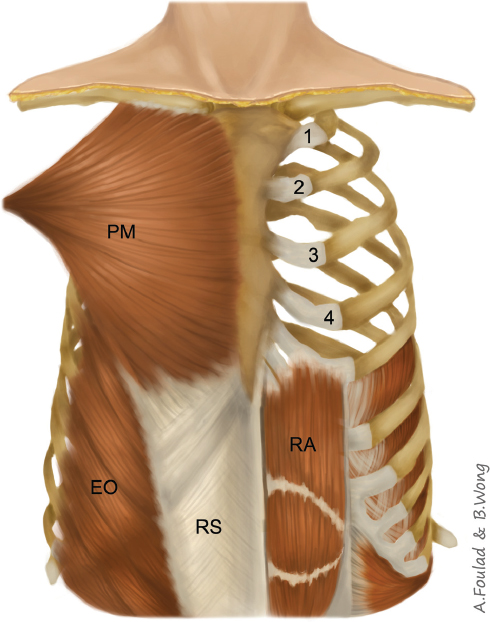
Deep to the skin and subcutaneous layers, the costal cartilages are covered by muscle ( Fig. 43.2 ). The upper costal cartilages are largely covered by the pectoralis major muscle which originates from the clavicle, sternum, superior seven costal cartilages (often does not include the first and seventh ribs), and external oblique aponeurosis. As the fibers of the pectoralis major muscle converge, a fanlike structure is formed that inserts onto the humerus. The rectus abdominis muscle is a more slender straplike muscle that extends over the lower costal cartilages as it originates from the pubic bone and inserts onto the costal cartilages of ribs 5, 6, and 7. Notably, a dissection of Asian cadavers revealed a main insertion onto the sixth rib, with no distinct fibers extending to the fifth rib. 13 Three layers of muscles are located lateral to the rectus abdominis muscle, which include, from superficial to deep, the external oblique muscle, internal oblique muscle, and transverse abdominis muscle. These muscles extend medially to form the rectus sheath that envelopes the rectus abdominis muscle.
Preoperative Planning
Preparing for costal cartilage harvest begins as early as the initial interview with the patient. A history of prior chest or abdominal surgery can significantly alter the surgical approach. If there is concern of prior excision or disturbance of the costal cartilages, the harvesting procedure should be directed at nonaffected regions, such as a different rib number or the contralateral side. If the patient has undergone placement of a breast implant, the surgeon should convey the potential risk of injury to the implant and also be attentive to avoid violating the capsule during the harvesting procedure.
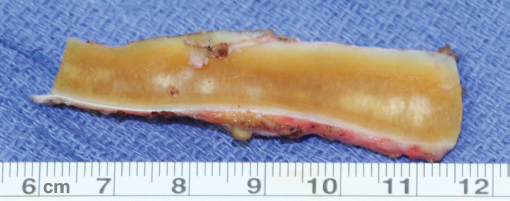
Radiologic imaging for assessing the costal cartilages may be helpful when there is concern for mineralization or abnormality. The presence of calcification causes cartilage to become more stiff and brittle, which can increase carving difficulty and potentially result in an unsuitable graft ( Fig. 43.3 ). Several studies have evaluated the degree of costal cartilage calcification as related to age and gender. 14 , 15 , 16 While the current literature does not enable precise guidance with respect to the degree of calcification as a discrete function of age, there is a general trend of increased calcification with age. Calcifications within the first couple decades of life are typically insignificant, while severe calcifications are more common during later years of life. Some surgeons consider obtaining computed tomography imaging of the chest in patients older than approximately 50 years of age. A more recent study, performed on an Asian population, revealed that female gender is associated with a greater calcification at a younger age. 17 Imaging may also be helpful for patients subjected to chest trauma, such as in boxers and professional football players. As an alternative to reduce cost and eliminate radiation, ultrasound may have a role in evaluating the costal cartilages. 18 Regardless of modality, the goal of imaging is to determine whether suitable cartilage for grafts exists and to aid in selecting the most appropriate costal cartilage to harvest.
Rib Selection
The grafts needed for the rhinoplasty influence the selection of the appropriate rib for the harvest procedure. It is imperative to obtain cartilage with a sufficient length and width for carving the desired grafts. An important principle is that the length of the costal cartilage typically increases from the first to seventh ribs, and then decreases after the seventh rib. For example, a study performed on cadavers of adults of Korean descent revealed that the average lengths of the fifth, seventh, and ninth costal cartilages are about 5.5 cm, 11 cm, and 6.5 cm, respectively. 13 The lengths of the straight portions of these costal cartilages measure about 5 cm, 9 cm, and 5.5 cm, respectively. It is the straight portions of the ribs that are most useful and versatile for carving grafts.
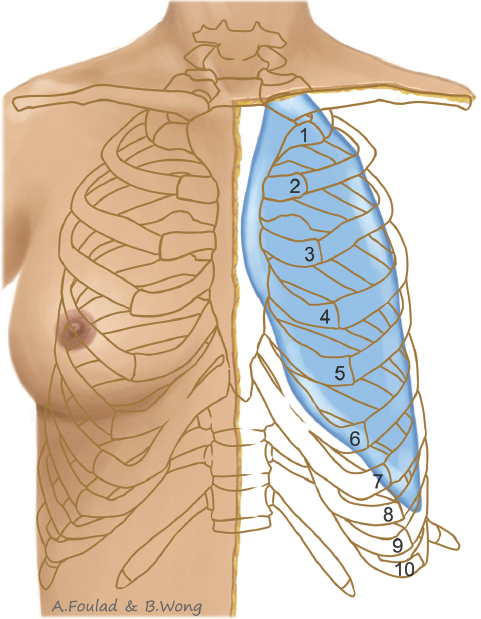
The fifth, sixth, and seventh costal cartilages are commonly used in rhinoplasty and can traditionally be accessed by an inframammary approach in females. A significant advantage is that the incision, which is typically made just above the inframammary fold, results in a scar that can be concealed by a bikini top or potentially by the breast itself. The approach is based on fairly consistent anatomy such that the medial aspect of the inframammary fold commonly overlies the fifth and sixth costal cartilages, and extends over the seventh rib more laterally ( Fig. 43.4 ). 19 Of these three ribs, the costal cartilage of the fifth rib is associated with the shortest length, but is favorable because it often has no attachment to adjacent costal cartilage. In comparison, the sixth and seventh costal cartilages join with adjacent costal cartilages, which increases the complexity of the harvest because of the necessity of having to split the attachments. A significant benefit of harvesting the seventh costal cartilage is that it has the longest length. 20 Furthermore, its more inferior position, compared to the fifth and sixth costal cartilages, places it within a safer location and may minimize the risk of a pneumothorax ( Fig. 43.4 ). 13 However, its farther distance from the inframammary fold increases the difficulty associated with accessing this cartilage through an inframammary incision.
Harvesting the costal cartilages of ribs 8, 9, and 10 conventionally requires a significantly inferior incision below the inframammary fold, such as through a subcostal incision that is more difficult to conceal. Albeit relatively difficult, the eighth costal cartilage can potentially be accessed via an inframammary incision. From a surgical standpoint, rib 9 is considered the first floating rib and does not have any significant attachments to the costal margin. This simplifies the harvest, and the dissection can be performed by starting from the medial free tip of the cartilage and extending laterally. Furthermore, harvest of the ninth and more caudad cartilages can be performed quickly with a supraperichondrial dissection, unlike the more cephalad costal cartilages that typically require a more meticulous subperichondrial dissection. 11 The size and shape of the 9th and 10th cartilages may also be more ideal for many rhinoplasty grafts. Compared to the cartilages harvested using an inframammary incision, these cartilages are smaller and require less carving. The decreased manipulation is felt to reduce carving time and potentially reduce warping. In addition, these ribs are also useful for harvesting osseocartilaginous grafts. The 11th costal cartilage is infrequently described in the literature, but its unique small size and simple harvest also has value as a graft source for rhinoplasty. 21
Incision Size
An appropriate incision length for costal cartilage harvest in rhinoplasty is usually between 2 cm and 5 cm. Long incisions are useful for obese patients due to a deeper dissection. Incisions limited to 2 cm or less can be attained with more experience. 11 , 22 These smaller incisions can be performed with commonly available equipment, but often limits access to the rib directly deep to the incision.
Endoscopic-assisted harvest has been described to help reduce incision length and improve incision placement within a more concealed region. In the literature regarding microtia repair, incision lengths under 2 cm have been used to harvest both the seventh and eighth costal cartilages from the same patient using a 4-mm diameter, 30-degree angle endoscope with a sleeve. 23 This technique involves drawbacks such as a prolonged learning curve, need for endoscopes, and operative times at least 1.5 times longer than conventional methods. A transumbilical approach has also been described to harvest costal cartilage up to 7 cm in length from either the seventh, eighth, or ninth ribs. 24 This endoscopic approach conceals the incision well, but requires a specialized skill set and significantly increases harvest time to about 2.5 hours.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


