4 Oncological Aspects of Breast Reconstruction
Summary
Despite the concern that immediate breast reconstruction (IBR) may delay the detection of local recurrence (LR) and the administration of adjuvant chemotherapy, there is no evidence that it has a negative impact on breast cancer survival. Conservative mastectomy, including skin- and nipple-sparing mastectomy, combined with IBR, have markedly improved the aesthetic results. Clinical evidence has not shown this conservative approach increases LR of breast cancer.
Complications of IBR have the potential to delay the administration of adjuvant chemotherapy. This emphasizes the importance of careful patient selection, especially in patients with more advanced, aggressive cancers. Postmastectomy radiotherapy treatment (PMRT) to reduce the risk of locoregional recurrence of breast cancer has a negative impact on all forms of breast reconstruction. There is abundant level III evidence that PMRT increases surgical morbidity including implant loss and capsular contracture. Autologous reconstruction appears to yield superior patient-reported outcome measures and lower risk of complications than implant-based reconstruction among patients receiving PMRT.
The use of contralateral prophylactic mastectomy in patients treated for unilateral cancer has increased in the last decade. It facilitates breast reconstruction, especially implant based. It has the potential for increase in surgical complications but has higher patient satisfaction than unilateral implant-based reconstruction.
Key Teaching Points
There is no evidence that immediate breast reconstruction (IBR) negatively impacts breast cancer survival.
Oncoplastic mastectomy improves the aesthetic results of IBR without an increased risk of local recurrence (LR) of breast cancer.
There is no data that support the routine surveillance imaging of breast reconstruction for LR.
IBR does not appreciably impact the administration of adjuvant chemotherapy.
PMRT has a negative impact on implant-based breast reconstruction. The body of evidence finds it increases capsular contracture and the risk of reconstructive failure.
Autologous reconstruction appears to yield superior patient-reported outcome measures and lower risk of complications than implant-based reconstruction among patients receiving PMRT.
Goals
There is no evidence that immediate breast reconstruction (IBR) negatively impacts breast cancer survival.
There is no evidence that oncoplastic mastectomy increases local recurrence.
IBR does not appreciably impact the administration of adjuvant chemotherapy.
Breast reconstruction makes the PMRT dosimetry more difficult.
There is no evidence that breast reconstruction increases the risk.
4.1 Introduction
Approximately 35% of women treated for breast cancer with total mastectomy receive immediate or early breast reconstruction. The percentage is higher in young women and those treated in tertiary care medical centers. Immediate breast reconstruction (IBR) has several advantages. It can prevent some of the negative psychological and emotional sequelae seen with mastectomy. The aesthetic results of immediate reconstruction are superior to those seen after delayed reconstruction. IBR also reduces hospital costs by reducing the number of procedures and length of hospitalization. IBR has the potential to impact the treatment of breast cancer. It could affect the delivery of adjuvant therapy and the detection and treatment of recurrent disease. Chemotherapy and radiation therapy could also impact the complication rates of reconstruction. The oncological considerations of breast reconstruction are outlined in this chapter.
4.2 Immediate Breast Reconstruction Impact on Survival
There are concerns that breast reconstruction may negatively impact breast cancer survival. Studies have shown that breast reconstruction does not interfere with the detection of local recurrences (LRs). Skin- and nipple-sparing mastectomy (SSM and SNM) are increasingly used to improve the results of breast reconstruction. Despite their relative surgical conservatism compared to traditional mastectomy, these techniques have not been associated with an increase in breast cancer recurrence. Complications after reconstruction have the potential to delay the administration of adjuvant therapy and potentially impact survival.
Agarwal et al used the Surveillance, Epidemiology, and End Results (SEER) cancer registry from 1998 to 2002 evaluated 52,249 patients to evaluate the breast cancer–specific survival of patients treated with immediate or early delayed breast reconstruction after mastectomy. Demographic covariates included age, race, marital status, income, education, county metropolitan status; oncological covariates included tumor stage, histological grade, lymph node status, hormone receptor status, receipt of radiation, and unilateral or bilateral mastectomy. Breast reconstruction patients had significantly lower hazard of death (hazard ratio [HR] 0.73, p < 0.0001) compared to those treated with total mastectomy alone when controlling for demographic and oncological covariates.
Access to breast reconstruction is a surrogate marker for quality of breast cancer care so these results are not surprising. Patients in cancer centers are more likely to be referred to plastic surgeons and undergo more aggressive treatment and surveillance in follow-up. There is also a selection bias that large multi-institutional cancer registries like the SEER registry cannot overcome. These registries do not collect data on patient comorbidities, which impact the selection process of who receives breast reconstruction. Healthier people are more committed to their medical care and are more likely to undergo breast reconstruction and ultimately have a better survival.
The effects of the stress of surgery including anesthesia, blood loss, and opioid use may impact cancer progression. Reconstructive surgeries, especially using autologous tissue, are longer operations with greater blood loss and postoperative pain. Studies are needed that examine the impact of different reconstructive techniques on breast cancer survival.
Pearl
Large population cancer registry had shown that immediate breast reconstruction does have a negative impact on breast cancer survival.
4.3 Immediate Breast Reconstruction and Local Recurrence of Breast Cancer
4.3.1 Skin-Sparing and Nipple-Sparing Mastectomy
SSM has markedly improved the aesthetic results of IBR (▶Fig. 4.1).
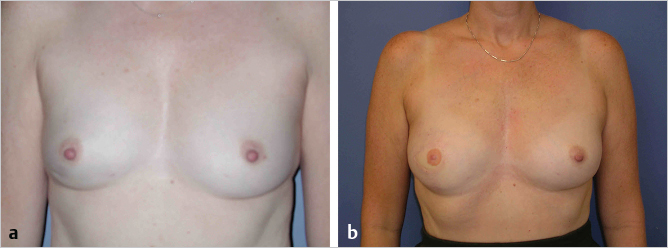
Preservation of the native skin envelope and the inframammary fold reduces the amount of tissue necessary for reconstruction. Breast symmetry can often be achieved without operating on the contralateral breast and the periareolar incisions are inconspicuous in clothes.
There have been concerns that the skin, nipple, and inframammary fold preservation reduce the effectiveness of total mastectomy. There is a large body of evidence that the LRs after SSM are comparable to non-SSM (▶Table 4.1). Care must be taken, however, in patients with superficial cancers or diffuse ductal carcinoma in situ (DCIS) to assure adequate surgical margins.
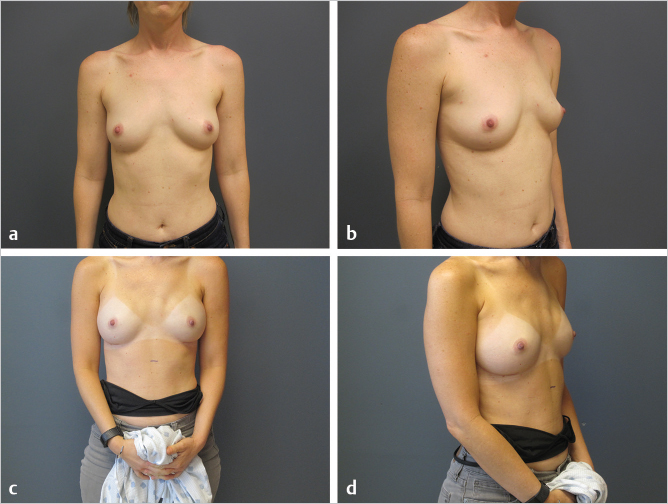
NSM is growing in popularity because of its perceived aesthetic benefits (▶Fig. 4.2). Patient satisfaction with nipple–areolar reconstruction following SSM can be disappointing. Data regarding the oncological safety of NSM are hampered by small sample size, varying indications and surgical techniques, and short follow-up (▶Table 4.2). There are limited oncological and reconstructive indications to perform NSM. Large tumors and those located in the central breast have an increased incidence of nipple involvement. Larger, more ptotic breasts are not good candidates for the procedure. Nipple elevation cannot be achieved without preservation of a dermoglandular pedicle, which impacts the completeness of mastectomy. The ideal candidate for a NSM has small-to-moderate–sized breasts with minimal ptosis.
Author | Year | N | Follow-up (months) | NAC recurrence |
Petit et al | 2005 | 579 | Median 41 | 0% |
Sacchini et al | 2006 | 68 | Median 24.6 | 0% |
Paepke et al | 2009 | 94 | Median 34 | 0% |
Babiera and Simmons | 2010 | 53 | Median 15 | 0% |
Kim et al | 2010 | 152 | Median 60 | 1.3% |
Jensen et al | 2011 | 77 | Mean 60.2 | 0% |
Warren et al | 2012 | 152 | Median 45 | 0% |
Lohsiriwat et al | 2012 | 861 | Median 50 | 1.3% |
Sakurai et al | 2013 | 788 | Median 78 | 3.7% |
Abbreviation: NAC, nipple–areolar complex. | ||||
Pearl
There is a large body of evidence that skin-sparing mastectomy does not increase the risk of locoregional recurrence of breast cancer. Nipple-sparing mastectomy is a relatively new procedure and varying indications and short follow-up hamper oncological outcomes data.
4.3.2 Detection of Local Recurrence after Breast Reconstruction
The role of postreconstruction imaging after the treatment of breast cancer remains controversial. There is a paucity of data that addresses the issue and there are no established guidelines. The incidence of LR of breast cancer is related to tumor stage. Most LRs after total mastectomy are in the skin and subcutaneous tissue and are readily detected by physical examination. A flap or implant could potentially delay the discovery of chest wall recurrences.
Systemic relapse is not inevitable following LR, especially after the treatment of DCIS. This argues that early detection of LRs may have a potential survival impact. All forms of mastectomy leave residual breast tissue. The differences are in terms of the microscopic breast tissue left behind in the skin and inframammary fold, which are largely preserved after SSM. Torresan et al evaluated residual glandular tissue in the skin flaps that would have been preserved after SSM. They found that 60% contained residual glandular tissue and it correlated with skin flap thickness.
The completeness of mastectomy is important in the treatment of DCIS because most cases of recurrence represent unexcised residual disease. Several authors have reported local recurrence of DCIS treated by SSM and IBR. They found that the majority of local recurrences were invasive carcinomas. This suggests that postreconstruction mammography can have a role in the early detection of recurrences prior to the development of invasive carcinoma.
Physical examination of implant reconstruction is relatively easy. There is minimal soft tissue covering the implant except along the inframammary fold and in the axillary tail. Deep chest wall recurrences are extremely unlikely because the implants are placed in the submuscular plane. Conventional mammographic evaluation has limited utility because the implants obscure soft tissue visualization. Magnetic resonance imaging (MRI), which has been used extensively to evaluate the integrity of silicone gel implants, may have a role in the selective surveillance after implant reconstruction.
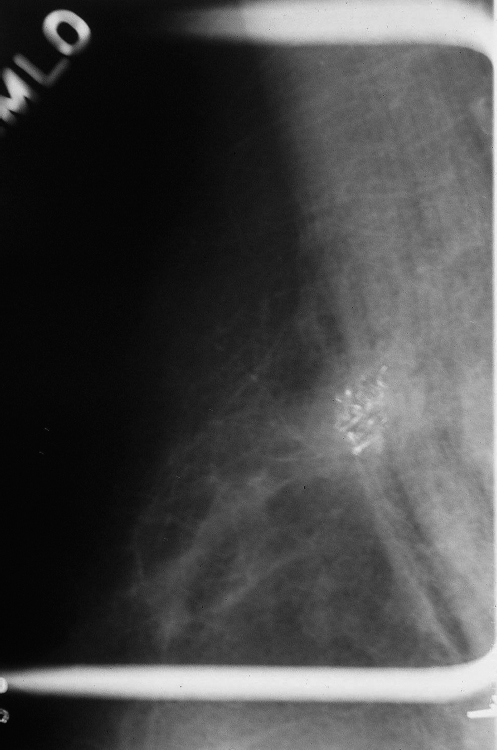
The sensitivity of physical examination of autologous reconstruction is lower than that seen with implant reconstruction. Deep chest wall recurrences often avoid detection until symptoms develop. Autologous reconstruction causes less impairment of mammographic tissue visualization. Benign mammographic findings after transverse rectus abdominis muscle (TRAM) flap reconstruction include fat necrosis, lipid cysts, calcifications, lymph nodes, and epidermal inclusion cysts (▶Fig. 4.3). Breast cancer recurrences in autologous tissue reconstruction are mammographically similar to that of primary tumors (▶Fig. 4.4). Proponents of surveillance mammography feel that screening breast cancer patients with autologous reconstructions can detect nonpalpable recurrences before clinical examination. Helvie et al evaluated surveillance mammography in 113 patients after TRAM flap reconstruction. Six patients underwent biopsy for suspicious mammographic findings and two LRs were detected. Two patients in the study group went on to develop recurrences that were detected by physical examination. There was one false-negative mammogram resulting in a sensitivity of 67% and specificity of 98% for surveillance mammography after TRAM flap reconstruction.

There is a paucity of data regarding the efficacy of MRI of the breast following autogenous breast reconstruction. Breast MRI has been shown to clearly delineate autogenous flaps from residual mammary adipose tissue. The absence of contrast medium uptake during breast MRI precludes recurrent carcinoma to a high probability. Fat necrosis in a TRAM flap will show early postoperative contrast enhancement, but this resolves within 6 to 12 months. Rieber et al evaluated MRI of the breast in the follow-up of 41 patients who had undergone autogenous tissue breast reconstruction. MRI was able to distinguish flaps from surrounding residual breast tissue in all cases. It excluded disease recurrence in four patients with suspicious mammographic or sonographic findings. It returned false-positive findings in three cases.
The potential indications for postreconstruction imaging include patients with close surgical margins and patients with diffuse DCIS treated by SSM. Its routine use after autologous reconstruction after SSM for invasive carcinoma warrants further study. The low detection rate and specificity do not justify the routine use of MRI in the follow-up of patients postreconstruction. MRI is most useful in patients with abnormal findings on physical examination or mammography and ultrasound. It is also helpful to delineate the extent of local disease recurrence.
Pearl
There is a paucity of data that supports the routine use of surveillance imaging of breast reconstructions.
4.3.3 Treatment of Local Recurrence after Breast Reconstruction
Surgical options following LR after breast reconstruction depend on the location and number of metastatic deposits and previous treatment. Imaging of the reconstructed breast and body scans are necessary to delineate the extent of tumor involvement (▶Fig. 4.4). Isolated LRs can be treated with removal of as much reconstructed tissue as necessary to achieve negative margins. Adjuvant chest wall radiation is usually administered (▶Fig. 4.5).

In cases of implant reconstruction, it may be necessary to remove a portion of the implant capsule necessitating implant removal in most cases. Howard et al reviewed 16 cases of LR after TRAM flap reconstruction. Eight recurrences occurred in the skin and were detected on physical examination. Eight recurrences occurred in the chest wall and were symptomatic, being detected on physical examination or diagnostic imaging. Twelve were felt amenable to surgical resection and three required removal of the entire TRAM flap.
Related posts:
 5 Gene Mutations and Breast Cancer Risk: Overview and Management
5 Gene Mutations and Breast Cancer Risk: Overview and Management
 10 Fat Grafting to the Breast in Prepectoral Breast Reconstruction—A Current Overview
10 Fat Grafting to the Breast in Prepectoral Breast Reconstruction—A Current Overview
 2 Breast Aesthetics
2 Breast Aesthetics
 1 Anatomy, Physiology, and Aesthetics
1 Anatomy, Physiology, and Aesthetics
 8 Fat Grafting in Breast Reconstruction: The Data
8 Fat Grafting in Breast Reconstruction: The Data
 9 Fat Grafting to the Breast: Aesthetic and Reconstructive Applications
9 Fat Grafting to the Breast: Aesthetic and Reconstructive Applications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


