38 Surgery of the Nasal Tip: Vertical Dome Division
Introduction
In recent years, three major trends have influenced the changes in nasal tip surgery. First, techniques have incorporated methods of greater medial stabilization and support of the nasal base. Second, more surgeons are relying on cartilage incisional and suture techniques of the alar cartilages rather than excisional ones to achieve desired changes. Finally, the use of the external approach for visualization of the alar cartilages has become commonplace, with the endonasal approach becoming an increasingly lost art form.
Philosophical Tenets of Vertical Dome Division
Ironically, the first two trends were longstanding philosophical tenets of Irving Goldman back in 1957. 1 Since his first published report on the importance of the medial crura and through subsequent articles on vertical dome division (VDD), 2 , 3 , 4 , 5 the message has been consistent: preserve and conserve rather than resect and regret. Yet the concept of incising the alar cartilage at the domal region has been labeled by many as dangerous, destructive, and radical rather than conservative and reasonable. It is vitally important not to combine excisional techniques and philosophy with an incisional procedure such as VDD. The complications of postoperative alar notching, collapse, unnatural tent-pole appearance, pinching, and bossae formation are caused more often by too much excision of the lateral crura than by dome division. 6
In almost all primary cases and in most revision cases, our approach to tip surgery is an endonasal one, using the marginal incision delivery technique. Sufficient delivery of this bipedal flap requires vestibular incisions at the caudal border of the alar cartilages and medial extension along 50% of the anterior columellar border. Attention to these details will allow a wide and adequate exposure to irregularities and asymmetries in the lobular tissues. More importantly, it will allow symmetrical incisions and suturing of tissue without the need for a transcolumellar incision. Insertion of additional filler or onlay cartilage in the lobular or columellar area can be easily accomplished via the marginal incisions.
Preoperative Evaluation
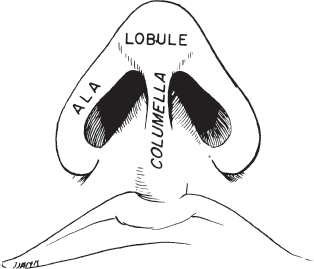
As with all rhinoplasty, preoperative evaluation of the nasal tip is critical in choosing the correct tip procedure. Decisions about where and when to incise cartilage and how much to remove are made during the preoperative assessment. With adequate tip projection, two factors are generally seen. First, the lateral view evidences a 1:1 relationship between the length of the base of the nose and the upper lip ( Fig. 38.1 ). Second, the base view shows a triangular orientation with an equilateral appearance, suggesting sufficient lateral battens of cartilage and strong medial support. The length and strength of the medial crura are evidenced in the ideal 2:1 relationship of the columella to the lobule ( Fig. 38.2 ). The desired double break occurs naturally from the retroussé curve of the medial crus at the columellar–lobular junction ( Fig. 38.3 ).

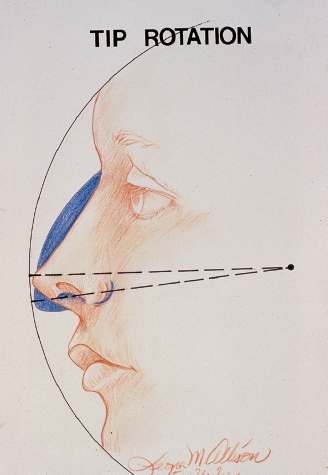
The cephalic movement of the nasal tip along the same radial arc from the facial plane defines tip rotation ( Fig. 38.4 ). Rotation is accomplished through the interrelated steps in rhinoplasty involving lowering of the nasal dorsum, shortening of the caudal septum, plumping of an acute nasolabial angle, and resecting the cephalic portion of the lower lateral cartilage. A conservative cephalic resection of alar cartilage alone does little to effect tip rotation. Also, overzealous resection leads to postoperative sequelae of alar collapse and nasal bossae.
Surgical Technique
Over the past 30 years, we have used various forms of VDD in more than 1,000 patients. The rationale behind VDD is the ability to change projection directly as well as to narrow and rotate the lobule with minimal cartilage excision. These desired effects can be accomplished without the use of additional struts or tip grafts because of the medial stabilization and strength provided by VDD techniques. Inherent in the philosophy is the preservation of surrounding tissues, such as the septal angle or caudal septum, further decreasing the risk of the postoperative appearance of an over-rotated or “overoperated” nose.
There are three distinct VDD techniques that are effective in addressing the nasal tip: the classic Goldman prototype, the Simons modification, and the hockey-stick modification. The indications and surgical technique for each of these procedures are discussed.
Goldman Technique
The prototype of VDD procedures is the classic Goldman technique, which calls for the creation of a chondrocutaneous strut by division of the alar cartilage along with the underlying vestibular skin. When employing the Goldman technique, the septal and dorsal alignment generally precedes the tip surgery. It is both crucial and advantageous that the initial lowering of the dorsum be minimal and that dorsal strength be maintained before the projection of the tip is changed.
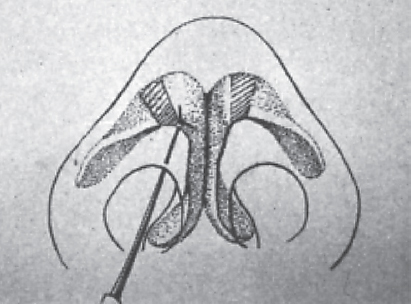
The alar cartilages are delivered through marginal incisions. The high point of the lobular apex is marked on delivery by a right-angled hook. It is important to remember not to borrow more than 2 or 3 mm from the lateral crus ( Fig. 38.5 ). The 3-mm borrowing boundary is measured along the caudal margin of the alar crus. The obliquity of the vertical cut at the dome allows more than 3 mm to be mobilized superiorly, thereby necessitating trimming of the posterior excess once the medial crura are brought together. The chondrocutaneous strut is sutured together with anterior, posterior, and superior horizontal mattress sutures of 4-0 chromic catgut ( Fig. 38.6 ).
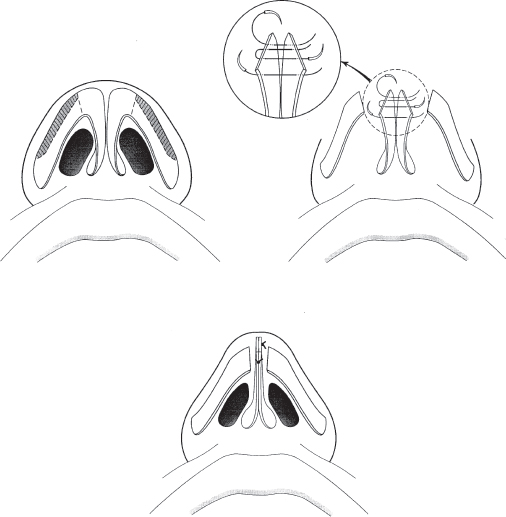
It is critical to preserve at least 8 to 10 mm of width of the lateral crura when trimming the cephalic border. It is worth reemphasizing that one should not borrow more than 2 or 3 mm from the lateral crus when dividing the dome vertically. Remembering these admonitions will help one to avoid the outcome of an unnatural tent pole appearance ( Fig. 38.7 ).
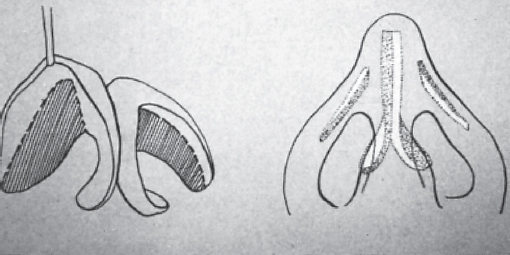
Sharp edges of cartilage are trimmed and the sutured crura are repositioned in the lobule. A final, high, securing suture closes the space between the caudal septum and membranous septum. No effort is made to suture medial crura directly to septum. The marginal incisions are closed and no attempt is made to suture the medial to the lateral crura ( Fig. 38.8 ).

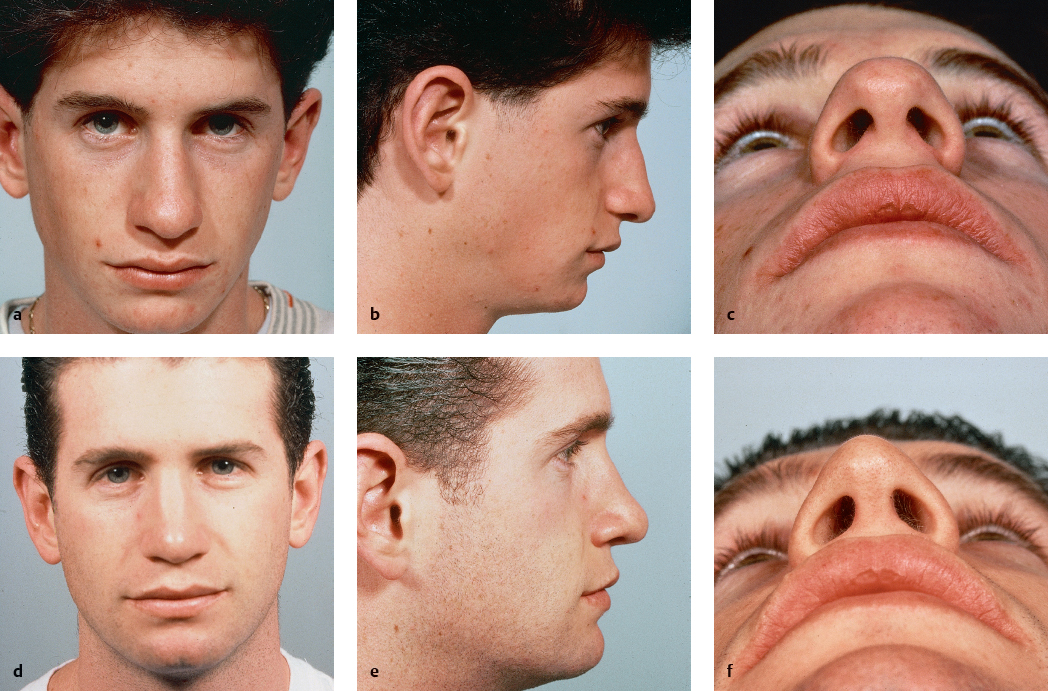
The Goldman technique is preferred by the authors for the ptotic or aging situation whereby the vertically displaced alar complex requires direct redirection ( Figs. 38.9 and 38.10 ). 7 If the nasolabial angle is particularly acute and the strength of the cartilage is suspect in regard to its ability to support the thick overlying skin, we often use a cartilaginous strut between the medial crura. Septal cartilage is generally used for the strut, which extends from the feet of the medial crura to the superior cut edges. This “sandwich” of chondrocutaneous leaves and cartilage is sutured together in the same manner as in the classic Goldman technique.

By rotating the medial crura together, the convex columella–lobular angle or so-called double break is at times created or accentuated. With a weaker, straight, or retracted columella, a cartilaginous batten or plumping grafts may further augment the tip procedure. Plumping grafts are small pieces of cartilage placed beneath the feet of the medial crura through a separate stab incision at the base of the columella. The cartilaginous batten is placed anterior to the medial crus via the medial aspect of the marginal incision (see section Adjunctive Techniques, below).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


