37 Surgery of the Nasal Tip: Endonasal Approaches
Introduction
With the advent of digital information, patients interested in nasal surgery have become increasingly more informed. Apart from the desired functional and cosmetic outcome, additional expectations are becoming increasingly more prevalent. The surgeon needs to discuss how postoperative downtime is minimized, when the patient’s appearance will have returned to inconspicuous, whether nasal packs are needed, when sports can be resumed, and whether the nasal tip will feel naturally soft to touch after the surgery. These aspects appear to be lending more justification to the use of less invasive approaches with decreased need for grafting and reduced collateral soft tissue trauma. Accordingly, the endonasal approaches appear to be experiencing a renaissance following their near complete disappearance with the tectonic shift toward the external approach in the 1990s.
Rhinoplasty is one of the most difficult procedures in facial plastic surgery, and endonasal tip plasty represents its most challenging part. The complex interactions of inner lining, skeletal elements, and the overlying skin–soft tissue envelope require an enormous degree of familiarity with anatomy, a wide armamentarium of techniques, as well as profound longterm experience to foresee outcomes. Just the exposure of skeletal elements like the lower lateral cartilages disrupts important soft tissue attachments, which contribute to shape and structure by tension banding effects along skeletal surfaces. The more extensive an approach, the more restorative maneuvers are hence required to maintain and preserve anatomical structure and physiologic function.
Endonasal approaches to the nasal tip are regarded as technically more difficult than the open approach, because the changes applied to the skeletal structures cannot be visualized without distortion. Advantages of the endonasal route include the availability of multiple approaches enabling the surgeon a more graded approach: the degree of soft tissue dissection can be incrementally adapted to the degree of correction required. Broader preservation of soft tissue attachments especially over the columella and infratip lobule can be achieved. Grafting over the tip and central pedestal is typically less extensive; swelling and edema may be less prolonged.
In terms of didactics, it is helpful to categorize the endonasal approaches according to the degree of soft tissue dissection required; they may be grouped into nondelivery, delivery, and complete release (extended delivery) techniques. The distinction between complete and incomplete strip techniques is another important parameter: it denotes whether the continuity of the lower lateral cartilages is preserved or interrupted. Table 37.1 lists the endonasal approaches to the nasal tip in order of ascending exposure, complexity, and potential to achieve profound changes.
For completeness, the external approach is also listed. The ability to assess the anatomical deformities of the nasal skeleton with minimal distortion and easier bimanual sculpturing under direct vision allows surgeons to approach and correct deformities of the nasal tip in earlier stages of their training. Disadvantages of the open approach include the need for more extensive grafting with donor site depletion, late soft tissue atrophy, and the creation of firmer nasal tips.
Facial Analysis
Before analyzing the typical nasal deformity, the surgeon should consider other major aesthetic components in the facial complex—forehead, eyes, lips, and chin—so as to create harmony and balance between these components. The aesthetics of the nasal tip are determined by shape, position, skin quality, and support. The shape is determined by the threedimensional configuration of the lower lateral cartilage, the position by rotation and projection, and the skin quality by texture and color. Support is determined by the structure of the skeletal components. Probably, tip support may be the most neglected of these aspects. Besides the important structural support of the central pedestal of the nose, the feel to palpation must be considered in postsurgical patients. Extensive grafting may result in an unnaturally stiff nasal tip, which does not show in photographs, but may be the cause of dissatisfaction for the patient.
Characteristics of the nasal tip in the frontal view (example of a postsurgical patient) include ( Fig. 37.1 ):

brow–tip line
tipdefining points
height and width of the tip
transition into the alar lobule
skin texture and color
in the lateral view ( Fig. 37.2 ):

tip projection and rotation
nasolabial angel
columellar show
columellar double break
and in the basal view ( Fig. 37.3 ):
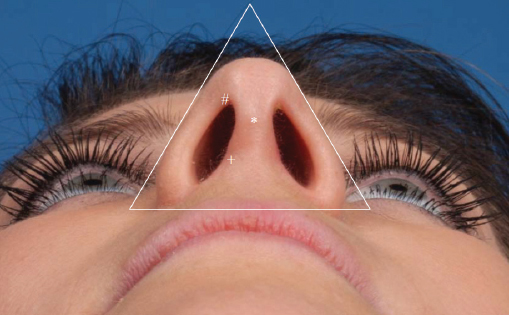
equilateral triangle of the tip
alar, tip, and infratip lobule
columellar base
nostril shape and size
Based on sound analysis, the surgeon must correlate the patient’s concerns and expectations with the deformities identified. Communication of realistic expectations is paramount for successful rhinoplasty. We use computer simulation as a routine during patient consultation. This tool allows the patient to understand the possibilities and limits of what surgery can achieve ( Fig. 37.4 ). Moreover, it allows the surgeon to develop a better understanding of the patient’s personality and level of expectation. The preoperative discussion should also include all aspects of pre-, peri-, and postoperative care.

Indications
The basic surgical approaches in endonasal tip surgery include the nondelivery and the delivery approaches. Among the delivery approaches, one may distinguish between complete and incomplete strip techniques. Complete strip techniques preserve the anatomical continuity and have a more favorable risk profile than incomplete strip techniques, which entail transection and overlapping suture of the lower lateral cartilage in various positions. Indications for each of these approaches depend on the specific anatomy of the nose and what proposed changes ( Table 37.1 ), including volume reduction, reconstruction, rotation, and change of projection, are planned. Moreover “softer” parameters like surgeon training and preference play an important role as well, which explains the lack of crisp selection criteria for one or the other approach with a given deformity. Variability is significant between surgeons, with some surgeons achieving substantial changes through less invasive approaches. Accordingly, the following discussion of indications can have orienting character only.
The Nondelivery Approaches: Indications
These approaches include the transcartilaginous and the transvestibular approach. The introduction of endoscopic techniques in rhinoplasty has extended indications for less invasive endonasal approaches. Authors, including Simmen, stress that control over dorsal contouring may be enhanced with high-definition endoscopic visualization. Behrbohm has developed specialized instruments that allow addressing dorsal irregularities very precisely, especially in revisional cases.
The Transcartilaginous Approach: Indications
Controlled cephalic resection of the lateral crus is completed with a transcartilaginous approach. As a result, reduction of vertical height of the nasal tip, rotation, and some narrowing may result. It is paramount to understand that the effects achievable with cephalic trimming are limited and overresection carries important risk of delayed nasal valve collapse, pinching, and overly accentuated horizontal alar folds. It appears that there is a trend in the literature toward more conservative cephalic trimming, and most authors recommend preservation of vertical height of at least 7 mm in females and 8 mm in males, with some authors recommending preservation of 10 mm in both genders. Techniques that can be applied through the transcartilaginous approach include intradomal sutures. Access to the dorsum is wider than with the transvestibular approach, allowing for easier modification of the middle vault and bony dorsum. See Fig. 37.7 for an example of the moderate amount of narrowing that can be achieved with this approach.
The Transvestibular Approach: Indications
The transvestibular approach, decribed by Fuleihan, is performed through a marginal incision. The vestibular skin is hydrodissected and subsequently elevated from the undersurface of the lateral crus. This allows for broad access to the undersurface of the lateral crus, enabling modification of the lower lateral cartilage through a variety of surgical techniques. These include cephalic trim of the lower lateral cartilage, moderate lateral advancement of the lateral crus, and interdomal and tipdefining sutures. The transvestibular approach allows moderate control of volume, width, and rotation of the nasal tip. It may be combined with other maneuvers like a tongue in groove technique to accentuate rotation and better control projection. Advantages of this approach include reduced soft tissue trauma and relatively quick recovery. Access to the dorsum may be somewhat more limited, and advanced maneuvers such as suture fixation of spreader grafts may be technically challenging.
The Delivery Approaches: Indications
The delivery approaches include the classic delivery of a bipedicled chondrocutaneous flap into the nasal vestibule and the complete release approach, which entails elevation of the vestibular skin off the undersurface of the lateral crus as well as transection of the piriform ligament. Delivery approaches allow direct visualization of the crural surface, including the domal and lobular segment of the medial crus. Modification of the domal angle can be achieved with suture techniques. The complete release approach offers the unique ability to control the position of the domal angle and to modify projection while maintaining a complete strip.
The Bipedicled Chondrocutaneous Flap Delivery Approach: Indications
The most important advantage of this (classic delivery) approach over the nondelivery approaches is that the superficial surface of the lower lateral cartilage is exposed and may be modified under direct vision. Exposure spans from the lobular segment of the medial crus medially to the lateral crus laterally. Compared to the nondelivery approaches, the bipedicled delivery approach allows for considerably greater changes to the shape of the nasal tip.
Typically, the lower lateral cartilages are exposed by retraction with a broad surgical instrument, which flattens and distorts the threedimensional structure of the cartilages considerably. This must be taken into account by the surgeon who needs to foresee the surface effects of surgical intervention on the nasal tip. Intermittent repositioning of the flap into the tip is helpful to judge the achieved changes.
A variety of techniques can be employed to modify the lateral crus. Tardy introduced the important concept of complete versus incomplete strip techniques. Complete strip techniques represent a more conservative philosophy. The anatomical continuity of the lower lateral cartilage remains intact. Changes are achieved by introducing or removing bends to the cartilage with suture techniques as well as conservative reduction of the vertical height and addition of grafts. Among the suture techniques frequently utilized are intradomal and interdomal sutures.
When vertical divisions of the lower lateral cartilage are performed in addition to the techniques listed above, an incomplete strip technique results. This is usually performed in order to achieve larger degrees of deprojection or when suture techniques are insufficient to remodel an overly wide, boxy, or divergent tip. Division of the lateral crus is best performed in its more lateral aspects where the thicker skin–soft tissue envelope reduces the risk of contour irregularities; this maneuver results in rotation and deprojection of the nasal tip. Division of the medial crus is typically performed at the lobular segment (Lipsett technique). This results in deprojection and derotation of the nasal tip. Divisions of the domal angle are propagated by some authors, while others discourage them. Overall, risks of all vertical divisions of the lower lateral cartilage include contour irregularities, asymmetry, and nasal valve compromise, especially in thinskinned patients. In terms of asymmetries and contour irregularities, the danger areas include the dome and the medial crus. In terms of nasal valve compromise, the central aspect of the lateral crus is most vulnerable. Reinforcement with stenting grafts such as alar batten or strut grafts may be indicated.
The Complete Release Approach: Indications
The complete release approach has resulted from efforts to avoid dome division, to preserve the anatomical continuity of the lower lateral cartilages, and to merge the structure approach of open rhinoplasty with the less invasive techniques of endonasal rhinoplasty. It is likely the technically most demanding and at the same time the most versatile among the endonasal approaches. It differs from the endonasal approaches described above in important aspects: it introduces the ability to completely reconfigure the shape of the domes and lateral crura. In order to better teach the concept, we utilize the model of a malleable metallic band that can be bent into various shapes. Such a band may be straightened and rebent into the desired shape without transection.
In analogy, the shape of the nasal tip is predominantly determined by the position and shape of the lower lateral cartilage and to a much lesser degree by the thickness and volume of the cartilaginous tissue. Hence, structural reconfiguration of cartilage has become the guiding principle, not resection. Key is the complete release of the lateral crus from all soft tissue attachments. Once this is achieved, compensatory advancement of the lateral crus gives room to position the domal angle in the desired position. With the addition of domal suture techniques and lateral crural strut grafts, the “old” domal angle is eliminated by structural grafting and a “new” domal angle is formed. Projection, width, and shape of the nasal tip can now be effectively controlled while division of the lower lateral cartilage is avoided. As the lateral crus is typically lengthened and stented with a lateral crural strut graft, there is a two-fold positive effect on the nasal valve: the lateral crus is (1) based laterally on a firm bony base—the piriform crest—and (2) structurally reinforced. Thus nasal valve pathologies can be both prevented and corrected. This applies especially to inward rotation of the cephalic edge of the lateral crus resulting from dome-approximating sutures. Moreover, the placement of an alar strut graft results in a straighter alar lobule, which has an important effect on cosmesis. The base view approximates the esthetic ideal of an equilateral triangle better and the alar lobule to tip relationship becomes more harmonious.
Aside from prevention and treatment of nasal valve pathologies, indications for the complete release approach include deformities that require dome divisions with other approaches: the markedly divergent, boxy, asymmetric, or overprojecting tip. Moreover, the complete release approach provides advantages in the treatment of the cleft nose deformity: it may be combined with extended premaxillary grafts and structurally firm caudal septal extension grafts. Thus, substantial projection of the central pedestal becomes possible without the risk of dehiscence of the transcolumellar incision. In summary, possible indications of the complete release approach include:
The broad, boxy, divergent, and bulbous tip
The over- and underprojected tip
Asymmetries of the nasal tip
Deformities of the tip associated with nasal valve compromise
Deformities of the tip associated with the cleft nose
The complete release approach is a recent addition to the armamentarium of endonasal approaches. It provides the experienced surgeon with great versatility and excellent tools for both cosmetic and functional improvement. However, it must be noted that the learning curve is long, and very precise execution is mandatory for excellent and safe results.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


