29 Posterior Trunk Disorders
Summary
Posterior trunk disorders can be congenital (e.g. myelomeningoceles) or acquired (e.g. pressure ulcers), and frequently require the expertise of plastic surgeons. Soft-tissue reconstruction is often required for wounds over the spine. Typically these defects are closed with local tissue; grafts and free-tissue transfer rarely are necessary.
Diagnosis of posterior trunk disorders is principally made by history and physical examination. Management is influenced by the depth of the wound, exposure of dura, infection, wound size and location, presence of hardware, duration of the wound, sensation and ambulatory status of the patient. The underlying cause of the wound must be addressed before considering operative interventions. For instance, pressure ulcers typically heal without operative intervention once the excessive pressure has been eliminated.
Myelomeningocele repair usually involves neurosurgical intervention in the first two days of life. Once the dura is closed, a plastic surgeon may be required to provide soft-tissue coverage for large defects. The reconstruction occurs in two planes: flaps over the dural repair, and skin closure. Regional muscles, perforator flaps, skin grafts, and skin flaps are all potential options.
The first line of management of pressure ulcers in the pediatric population involves periodic weight shifting, and specialized wheel-chair cushions and beds for non-ambulatory patients. It is important to investigate the cause of the wound and to eliminate the etiology. Whilst conservative therapy is the mainstay of treatment, operative closure is sometimes required. Other posterior trunk disorders, such as wounds over the spine and traumatic soft-tissue defects, are also managed by plastic surgeons.
29.1 Introduction
Posterior trunk disorders can be congenital or acquired. The most common malformation plastic surgeons are asked to manage is myelomeningocele. The most frequent acquired defect is a pressure ulcer. Plastic surgeons often are asked to reconstruct soft tissue for wounds over the spine. Generally, posterior trunk defects are able to be closed using local tissue; grafts and free-tissue transfer rarely are necessary.
29.2 Diagnosis
Diagnosis of posterior trunk disorders is made by history and physical examination. Imaging and histopathology are rarely indicated. Variables that will dictate treatment include the following: (1) depth of wound, (2) exposure of dura, (3) infection, (4) wound size and location, (5) presence of hardware, (6) duration of the wound, and (7) sensation and ambulatory status of the patient. If a wound has been present for at least 6 weeks, then it is chronic and likely has not healed because of infection, bacterial colonization of hardware, or pressure. The underlying cause of the wound must be addressed before considering operative interventions.
29.3 Nonoperative Treatment
The surgeon managing a posterior trunk disorder should begin considering reconstructive options as low on the reconstructive ladder as possible. Pressure ulcers typically heal without operative intervention once the excessive pressure has been eliminated. Superficial wounds can be allowed to heal secondarily. Before considering operative intervention, the benefits of the procedure must outweigh its risks.
29.4 Operative Treatment
29.4.1 Myelomeningocele
Myelomeningocele is the most common neural tube defect affecting approximately 1/3,000 children. The spinal cord is exposed due to a cleft in the vertebral column and overlying soft tissue. The repair is usually performed on the first or second day of life to prevent cord desiccation and meningitis. After the neurosurgeon detethers the spinal cord, infolds the placode, and closes the dura, he/she may ask for a plastic surgeon to provide soft-tissue coverage if the defect is large. Several methods have been described to reconstruct tissue over the dural repair: regional muscles (latissimus dorsi, gluteus maximus), perforator flaps, skin grafts, and skin flaps (bilobed, bipedicle, rhomboid, rotation, V-Y advancement).
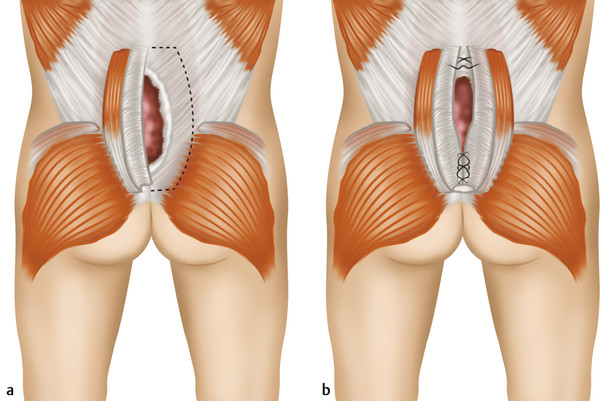
I believe the best method to manage a myelomeningocele is to reconstruct the area in two planes: (1) flaps over the dural repair and (2) skin closure (Box 29.1). First, I use turnover paraspinous fascial flaps to cover the dural repair (Fig. 29‑1 and Fig. 29‑2). The flaps are elevated laterally to medially, turned over, and sutured in the midline with interrupted 4–0 vicryl. Hydrodissection with local anesthetic lifts the fascia off the underlying muscle facilitating the dissection. The paraspinous fascia provides a strong, tension-free, vascularized layer over the dural repair. The thick tissue reinforces the dural incision line to reduce the risk of cerebrospinal fluid leak. The fascial flaps separate the dural and skin closure to reduce the risk of cerebrospinal fluid contact with the integument and meningitis.
Box 29.1 Principles of Extradural Myelomeningocele Reconstruction
Paraspinal turnover fascial flaps
Cover the dura and decrease cerebrospinal fluid leak
Separate dural repair from skin closure
Avoid gluteal/latissimus flaps, which can defunctionalize a neurologically compromised patient
Linear midline skin closure
Reduces complications
Facilitates reoperations for tethered cord and scoliosis

This technique does not include muscle dissection and thus will not worsen the functional deficit in a neurologically compromised patient. The patient’s ambulatory status is related to the level of spinal involvement. Ninety-five percent of children with L5 or sacral myelomeningocele are able to ambulate moderate distances (community ambulators). Patients with defects at L3 or above are only able to ambulate short distances (nonfunctional ambulators). Sixty percent of patients with myelomeningoceles will be community ambulators, 15% nonfunctional ambulators, and 25% are nonambulatory. Paraspinous turnover fascial flaps obviate the need to use major muscle flaps (e.g., gluteal, latissimus), which are more complicated to dissect and have a greater risk of complications. Harvest of gluteal and/or latissimus muscles also can further defunctionalize an infant with a myelomeningocele. Use of gluteal muscle flaps in a potential community ambulator may cause the child to become a nonfunctional ambulator or nonambulatory. Harvest of latissimus muscle will handicap a child’s ability to walk with crutches and/or transfer from a wheelchair.
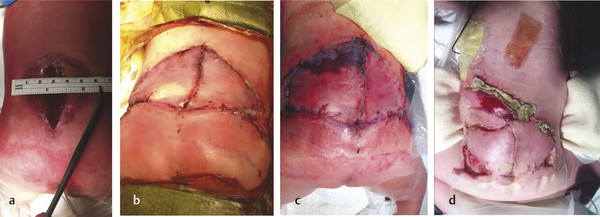
After providing deep soft-tissue coverage over the dural repair with paraspinous fascia, the overlying skin is approximated. To approximate the integument, skin flaps are widely undermined above the muscle fascia, advanced medially, and sutured vertically in the midline over two drains with interrupted 4–0 vicryl and 4–0 nylon suture. If large defects are closed with tension, prone positioning is prescribed for a minimum of 2 weeks postoperatively and the nylon sutures are maintained for at least 4 weeks.
Skin closure in the midline is important for myelomeningocele repair because patients often require additional operations involving the posterior trunk. Secondary procedures for cord tethering or spinal fusion for scoliosis occur in one-half of patients. I avoid the use of bilobed, bipedicle, rhomboid, rotation, or V-Y advancement flaps to minimize posterior trunk scarring and complications (Fig. 29‑3). The vertical scar facilitates exposure for secondary spinal procedures and minimizes the risk of skin necrosis from multiple posterior trunk incisions. Wide skin undermining will achieve a linear, midline closure without breakdown for even the largest defects. If the incision line separates, it will heal secondarily without consequence; the risk of meningitis is small because fascial flaps separate the integument from the dura.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


