26 Facial Rejuvenation Using Energy Devices
Pearls
Collagen denaturation is one of the mechanisms for nonablative rejuvenation laser treatment.
Cooling during nonablative facial rejuvenation is very important for the skin of East Asians.
Energy devices that do not use light may be safer in Asian skin. Pigmentation in the epidermis of Asian skin hinders effective delivery of light into the dermis and causes complications such as hyperpigmentation. Energy devices that do not use light have no interaction with epidermal melanin.
Energy device emissions other than light can bypass epidermal melanin tissue, but Asian skin reacts immediately to inflammation caused by skin damage and may develop hyperpigmentation even when a light source is not used for rejuvenation.
Depending on the nature of the energy device, surgeons can target different depths for rejuvenation. Sometimes multilayer therapy is possible with the combined use of these devices.
Infiltrative radiofrequency (RF) can target different depths by changing the lengths of the needles, thus facilitating multilayer therapy.
Intense pulsed light (IPL) is very useful for type I rejuvenation. But it should be used with caution as it has a large spot size and complications can be catastrophic.
Among the types of fractional laser treatment, superficial treatment lasers such as the thulium fractional laser give immediate effective results. Because it targets the surface, the changes are readily visible. This phenomenon doesn’t imply that shallow treatment is better than deep treatment.
To reverse aging beyond the depth of the skin, highintensity focused ultrasound (HIFU), infiltrative RF with long needles, or interstitial lasers can be applied.
HIFU was originally introduced to tighten the superficial musculo-aponeurotic system (SMAS) and may destroy fat when delivered to the fat layer. This can be used very effectively for chubby cheeks.
Introduction
Skin rejuvenation is an aesthetic procedure to counteract or reverse signs of the aging process such as pigmentation, vascular ectasia, wrinkle, and loss of elasticity. Skin rejuvenation can be divided into two types. Type I rejuvenation reverses skin problems such as dyspigmentation and vascular changes, while type II rejuvenation aims to reduce wrinkles and restore skin elasticity. Ablative versus nonablative rejuvenation is a concept different from type I and type II rejuvenation. Ablative rejuvenation is used to target photo-damaged skin that progressively worsens with age. Through the ablation of the epidermis and portions of the superficial dermis, as well as the induction of collagen remodeling in the deeper dermis, ablative resurfacing can reduce wrinkles, dyschromia, skin laxity, and vascular changes. On the other hand, nonablative rejuvenation delivers heat to the epidermis, dermis, and subcutis without epidermal damage, thereby inducing collagen denaturation. Either an ablative or a nonablative method could be either type I or type II rejuvenation.
General Principles
Principles of Nonablative Rejuvenation
The aims of nonablative rejuvenation (NAR) are to reduce wrinkles and to increase elasticity. NAR includes not only type II rejuvenation without ablation of the skin, but also type I rejuvenation, which can be achieved by IPL, Q-switched laser, or dye laser. NAR delivers heat to the epidermis, dermis, and subcutis using lasers or radiofrequency. Since NAR treatment does not cause epidermal damage, it is safe and allows a rapid recovery, with less chance of the hyperpigmentation and prolonged erythema that is associated with laser peeling. NAR includes various lasers and radiofrequencies. Based on the chromophores that interact with each laser, the NAR lasers can be classified into three categories: (1) dye lasers, which use hemoglobin as a chromophore; (2) Nd:YAG lasers, which use hemoglobin, melanin, and water as chromophores; and (3) midinfrared lasers, which use water as a chromophore.
Most lasers for NAR use water as a chromophore to generate heat in the skin. Wavelengths between 1,300 and 1,600 nm are used for this purpose. Within this range, the wavelength that has high absorption to water can penetrate the skin more shallowly than the wavelength that has low absorption to water. Using these characteristics, appropriate wavelengths can be chosen to heat the exact depth of the skin. Fractional treatment, a nonablative type, also uses a wavelength between 1300 and 1600 nm, and determines its depth of penetration according to the wavelength. The key mechanism of NAR is collagen denaturation, which results in regeneration of new collagen. Generally, collagen exposed for more than 1 second to 60°C showed denaturation. But when it was exposed to a temperature less than 50°C, activated heat shock protein (HSP) increases the collagen synthesis rather than denaturation.1,2 In the case of dye laser treatment, collagen fibers showed changes after 2 weeks and increased collagen fibers appeared after 4 weeks. After 5 weeks, an increased number of fibroblasts was conspicuous.3 A light-emitting diode (LED) was also able to demonstrate increased activity of fibroblast without collagen denaturation.4 CO2 lasers, dye lasers, and NAR treatments are also known to increase matrix metalloproteinases (MMPs), which remove photo-damaged collagens and result in the activation of fibroblasts, thus contributing to the reversal of the aging process.5,6 Collagen synthesis was apparent in 1 to 2 months and the result persisted up to 1 year.7 On the other hand, the effect of treatment with ablative fractional CO2 laser was maintained from 3 months to up to 2 years.8,9 This implies that ablative laser is more effective and the effect is longer-lasting compared with the nonablative laser in terms of collagen synthesis.
Principles of Ablative Rejuvenation
Beyond tissue ablation, short-pulsed, high-energy, rapidly scanned CO2 lasers are able to tighten the skin by means of two mechanisms: controlled instantaneous heating and wound healing.10 Precise heating of collagen leads to immediate contraction and visible skin tightening from destruction of the hydrogen bonds within the collagen triple helix without destroying the collagen molecule. The ideal temperature has been shown to be 63°C. As temperature rises, more and more cross-link bonds are broken until denaturation and loss of structure occur. Denatured collagen sloughs in the first few days after the procedure with full re-epithelialization within 1 week. Over the ensuing 3 to 6 months, this process stimulates new collagen deposition and fibroblast proliferation. The wound healing response induces contraction through fibroplasia. This ablative fractional treatment has a higher risk of complications, but the effect of treatment is superior. Modern fractional ablative technology allows for ablation of a portion of the epidermis while leaving adjacent, untreated skin to act as a reservoir for healing, resulting in a shorter downtime and lower risk for complications.
Concept of Type I and Type II Rejuvenation
For type I rejuvenation of Asian skin, IPL, Q-switched lasers, chemical peeling, and medical skin care, including vitamin C iontophoresis, can be used. Although medical skin care requires longterm treatment, it is safest and very useful when combined with other treatment. Vitamin C iontophoresis is often used before and after laser treatment. Patients with sensitive skin can get type I rejuvenation safely with IPL as opposed to chemical peeling. Normal skin treated with chemical peeling may respond positively, showing improvement in both pigmentation and wrinkling. The Q-switched laser is the standard laser for pigmentation problems. It targets specific lesions and has a small treatment beam size, whereas IPL has a very big spot size.
For type II rejuvenation aimed at improving the appearance of wrinkles, various kinds of lasers and energy devices can be applied. To reverse epidermal aging, ablative or nonablative fractional lasers and infiltrative fractional RF can be used. In Asian skin, the ablative lasers are subject to complications such as hyperpigmentation, and so the nonablative fractional laser is safer. For dermal reform, LED, pulsed dye laser, NAR and fractional lasers, and infiltrative fractional RF can be used. Infiltrative fractional RF bypasses the epidermis with cold penetration needling, so it could be a good option for Asian skin, which easily develops hyperpigmentation. The same factor renders RF useful for patients who have sensitive skin. Reduction of fat volume in the subcutaneous fat and tightening of SMAS are possible with monopolar RF, HIFU, and interstitial lasers.
Commonly Used Devices in Facial Rejuvenation
Devices used in facial rejuvenation can be divided into four groups based on energy source: light, radiofrequency, ultrasound, and pneumatic. Light-based devices include the dye laser, IPL, Nd:YAG laser, midinfrared laser, fractional laser, and interstitial laser. Radiofrequency devices are divided into monopolar, bipolar, and infiltrative types using the electrical current through a treatment tip. Recently, ultrasound and microjet injection by pneumatic compression are being used as noninvasive methods.
Rejuvenation by Light Devices
Dye Laser
The pulsed dye laser uses the wavelength of 585 to 595 nm. It targets hemoglobin in the capillaries of the dermis, indirectly stimulating the dermis. The conventional pulse duration of 0.45 ms produced purpura, but low-energy treatment with an NLite laser (Clemson Eye) with pulse duration of 0.35 ms showed effectiveness with no purpura.11
Intense Pulsed Light
Intense pulsed light, or IPL, is broadband light, as opposed to a a laser, that emits light with a single wavelength. The spectral distribution is between 550 and 1200 nm. Various wavelengths interact with various chromophores in the skin, and generally longer wavelengths penetrate deeper. Because broadband light has diverse effects on the skin, selectivity toward a certain target is low compared with laser. There are various kinds of IPL with different spectral distributions, spot sizes, etc. The parameter shown on the computer screen, however, may not be the real IPL beam parameter. Therefore, using the same parameter between different IPL devices is unreliable and should be avoided.
Type I Rejuvenation with IPL
Treating a vascular lesion with IPL risks heating melanin pigments at the same time due to the broad spectrum of the light. When using IPL to treat vascular lesions, blisters and crusts are seen before the development of purpura. Blisters and crusts are manifestations of epidermal heat damage. Multiple pulses of IPL can generate heat around the vessels. Therefore, epidermis must be given time to cool down. This can be achieved by allowing a longer thermal relaxation time than the interval between subpulses of IPL.
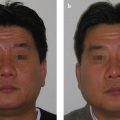
As for treatment of pigmentation, IPL has a long pulse duration, which leads to mild changes after treatment. It heats up and produces mild changes in a melanocytic lesion without melanosomal destruction. By selecting the appropriate filter, the optimal setting for each skin phototype can be achieved. When IPL is used for the treatment of melasma, special adjustment of the parameters is necessary. The parameter used for the treatment of melasma is lower compared with other pigmentation problems. Inadvertent high fluence irradiation on melasma can lead to aggravation of this condition. This phenomenon typically manifests in the case of invisible melasma or mild melasma masked by other pigmentation problems. Since IPL treatment uses a very large spot size compared with lasers, it is suitable for obscuring the dyspigmentation in the whole face and achieving general improvement (Fig. 26.1).

Depending on the site of the face, however, the optimal setting can vary dramatically. Areas such as the forehead, mandibular line, and zygoma should be treated cautiously. These areas overlying the facial bones are prone to erythema and pain. The forehead should be treated with a fluence at least 2 J/cm2 lower than the settings used to treat the cheek. During IPL treatment, cooling gel is useful to prevent formation of air space between the treatment tip and skin surface. Filling the space with gel can help propagate light evenly into the skin. The gel can also help to cool down the treatment tip, which becomes hot with continuous firing of IPL. Depending on the thickness of the gel, the attenuation of light can be changed. More than 10% attenuation is expected with the use of gel. Hence, it’s essential to know the thickness of the gel applied. It is more likely to find curved areas such as the nose and forehead better covered by the gel. When the assumption is that the gel is too thick and the parameter is adjusted to compensate for the attenuation by the gel, overly high fluence may be delivered. If the attenuation is not as expected, this may become dangerous to the patient. It is therefore safer to set the parameter with the assumption that the layer of gel is thin. Some operators may attempt to push the crystal closer to the skin surface. This would not increase the fluence delivered to the skin, though any possible complication would be negligible. In any case, the thickness of the gel should be kept constant at all times.
Immediately after irradiation, the pigmented lesion may become darker, which indicates adequate treatment. The treatment end point should be controlled carefully. Immediately after IPL irradiation, the skin shows mild erythema. That is generally regarded as a treatment end point. When the redness is diffused, it is fine; but the situation is dangerous if the redness is intense and shows the mark of the treatment tip. This ill-defined erythema usually subsides in several minutes. The erythema is not the only signal for completed treatment. To predict the optimal treatment end point, various factors should be taken into account such as pain, color change in pigment after treatment, skin type of patient, outdoor activity, patient’s general condition, and gender.
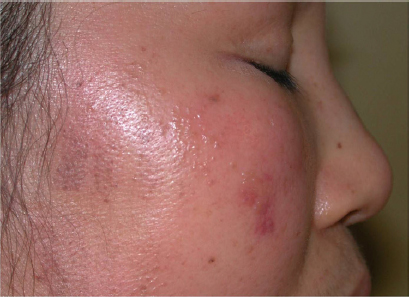
One of the common complications of IPL treatment are rectangular crusts. The mild cases spontaneously subside. A crust is a problem when it becomes big and visible. After the crust falls off, redness persists for several months. Generally, the most serious complications of IPL treatment are blisters, crusts, longlasting erythema, and hyperpigmentation (Fig. 26.2).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


