23 Management Strategies for the Aging Asian Face: Philosophy and Evolution
Pearls
The principal manifestation of aging for most East Asians (and all other peoples for that matter) is volume loss. Judicious volumization using fat grafting and/or fillers can provide wonderful rejuvenation that is natural and impactful.
Hair restoration can be a vital component to global facial rejuvenation and can provide an important frame to the upper face to make it appear more youthful and attractive.
The aging Asian eyelid is a complicated subject. The treatment algorithm is based on which type of eyelid a patient possesses: a natural eyelid crease, an eyelid without a crease, or an eyelid with a previously surgically created crease.
Typically, lower facial rejuvenation for the East Asian is not necessary until much later in life when compared with the Caucasian. Neuromodulators can be used in the platysma to reverse early aging and to delay the need for a facelift. A chin implant can be an important adjunct to improve the shape of the Asian face as well as to enhance a facelift result. Lipocontouring of the neck should be done sharply with scissors in a conservative fashion under direct vision rather than with a suction cannula.
Management of the skin should be an integral part of every consultation and strategy for global rejuvenation. However, it is advisable to always be more conservative when it comes to ablative techniques owing to the increased risk and time of convalescence for the Asian patient.
Introduction
The aging East Asian face bears remarkable similarities to the aging faces of other peoples, but also has distinct attributes that separate it from the rest of the world. This chapter will explain both the similarities and differences of the Asian face regarding the aging process and how to approach it in a culturally sensitive, effective, and safe manner. The focus of the chapter will be heavily biased through the filtered lens of my worldview, which I hope will increase the pragmatism of the content rather than be considered overly simplistic or prejudiced.1,2,3 The major topics that will be covered include hair restoration, facial volumization, Asian blepharoplasty,4 and facelifting. To cover each of these topics surgically would take a textbook to do the subject matter justice. Instead, this chapter will focus on the relevant aging process of the Asian face on a global scale and touch on the philosophy of what ages the Asian face and how in general terms to manage this problem. I believe that this chapter will be helpful both for the surgeon who is new to working with the East Asian face and for the surgeon who has great experience in this field.
Patient Assessment and Philosophy of Aging
The Asian face has been considered relatively resistant to the aging process, at least compared with the fairer races, who are more subject to the weathering effects of solar exposure. The unique nature of the Asian’s skin stands as a barrier to the detrimental effects of solar rays and helps keep the face from the accelerated aging that is a common and early feature of many Caucasian faces.5 Nevertheless, aging does occur both subtly and profoundly but perhaps not so aggressively as in the Caucasian. Part of this protracted youthfulness in the Asian can be attributed to the cultural proclivity to avoid the sun for two principal reasons. First, sunspots and freckles that may be considered charming in the Occident are often deemed unattractive in Asia. Second, the darker skin that an Asian bears may relegate the individual to a lesser societal status, whether overtly or subconsciously. This bias toward fairer complexion reigns in many cultures throughout Europe, Africa, and many other sectors of the world. I believe that sun exposure can actually be worse for aging than smoking or other nicotine use, and that sun and nicotine together can be negatively synergistic. Further, Asians who remain in Asia typically have healthier diets than those Asians who migrate to the West, which can further maintain their youthful mien. All bets are off when the Asian decides to travel to the West to settle and then adopts Western habits of sunbathing and consumption of processed and heavily adipose-laden foods. Nevertheless, the genetic nature of the Asian skin type can provide relative protection against aging despite the adoption of such adverse lifestyle changes.
Volume Loss and Volume Restoration
Even though Asians age relatively less than their fairerskinned counterparts, there are still unmistakable signs of aging in the Asian face. It would be quite rare to look at a 70-yearold Asian and unwittingly assume that she is only 30 years old. If her skin (like that of many of my octogenarian aunts) is relatively white, unblemished, and almost wrinkle free, why is it so obvious that she is indeed much older? To me, the answer is readily apparent. It is the universal sign of volume loss that affects all races in relative degrees but is the predominant feature of the aging Asian face.6
Volume loss is observed as a linear loss of fat from birth until death. A 1-yearold has considerably more facial fat than a 5-yearold. Similarly, a 5-yearold’s face has more fat than a 10-yearold’s. In an adult if body weight is held the same, every 5 years represents ineluctable, progressive volume loss and skeletonization of the face. Accordingly, the senescent shadows that develop across the face and the loss of glorious, youthful highlights should be the principal targets in revolumizing the face. Further, there is an immediate “blink” effect: We pretty much know who is young and who is old in a nanosecond, based on facial shape. A young face is very round, which we have a special term for: baby fat. Baby fat is nothing special. It just represents the exuberant fat of youth that gradually dissipates. As youth regresses, the shape of the face becomes a more angelic oval by 30 years of age, which is cherished by many women who fear looking fat as the ideal age of beauty. By 40 years of age, as the fat continues to skeletonize and the malar bones begin to be partially exposed, the face becomes squared off in appearance. Further volume loss and possibly some weight gain contribute to an inversion of the facial features, where the lower face increasingly becomes the dominant attribute. Accordingly, a primary focus for the aging Asian face is to restore balance and shape to the face to make it look more youthful. I believe that filling the temple, periorbital region, malar area, and perioral area can be as helpful for the Asian face as it is for other ethnic and nonethnic faces, with a few caveats.
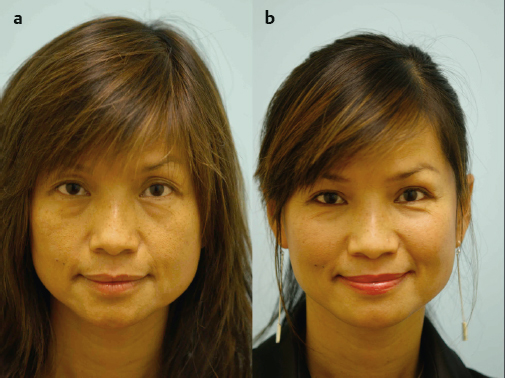
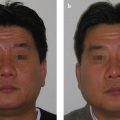
First, Asian faces in general tend to be fuller to begin with than many white faces. Therefore, it is important when filling an Asian face not to do so as robustly in many cases as for the very gaunt faces that are often seen in other races. In fact, filling areas around the periorbital and chin regions can make a face actually appear slimmer if done in a judicious fashion (Fig. 23.1). A further word of caution is that in many Korean faces, filling the malar region can be deemed masculinizing since it can square off a wide face; in fact, many Koreans pay to have their malar bones surgically reduced and collapsed inward. This cultural sensitivity should be verbally addressed and heeded to avoid a miscalculated outcome.
There are two principal mechanisms for volumizing a face, fat grafting (a surgical modality) and injectable fillers (an in-office procedure). Fat grafting is very effective as a durable, longlasting result but suffers from a few drawbacks. First, absorption is relatively unpredictable. There can be variable loss of the transplanted fat, though in general there should be a large percentage that remains. Accordingly, I do not like to use fat grafting to try to fix one area of the face since the absorption rate may compromise the intended outcome. Conversely, if the entire face is treated, sufficient fat grafting can survive so that the entire face appears better. Such an instance, when enough of the transplanted fat is left to contribute to an improved look of the face, may be called an improvement in one’s “blink”; that is one looks better in the blink of an eye to an onlooker even though the minutiae of the face may not be entirely corrected in every way. I use fillers to touch up almost any fat graft to achieve improved outcomes.
If fillers can be so accurate in rejuvenating the face, why is this method not preferred over fat grafting? The simple reason is cost. Fat is free; it can be harvested without paying for each syringe except for the labor that is involved. Fillers, especially durable fillers like poly methyl methacrylate, can be costly when multiple syringes are used to contour every detail of the face. Today, with the advent of disposable microcannulas, I have had an exponential increase in the use of fillers because many patients do not prefer the up-front cost, the nature and time of the recovery process, and the variable absorption of fat grafting. When approaching a face with either fillers or fat grafting, I prefer to target a little bit of filler or fat at almost every small area of the face, including the temple, brow/upper eyelid, lower eyelid, nasojugal groove, anterior cheek, lateral cheek, subzygomatic recess, buccal area (as deemed appropriate), canine fossa and nasolabial groove, prejowl sulcus, anterior chin, and lateral mandible (as deemed appropriate). By filling all of these areas, the face appears balanced and rejuvenated. The degree and distribution of the filler are based on artistry, judgment, and experience and lie beyond the scope of this philosophically based chapter.
Hair Loss and Hair Restoration
Hair restoration occupies a large part of my clinical practice, and I have extensive experience working with the Asian patient. I will speak here again in terms that are specific to the Asian, and also present some universal concepts that can be helpful for anyone who is contemplating entering the field of hair transplant surgery. Further, to elaborate on every technical aspect of how to perform hair restoration would be nearly impossible in a span of a few pages, and any cursory treatment of the procedure would not do it justice. Nevertheless, the artistic and philosophical points are well worth exploring even in the format of this chapter.
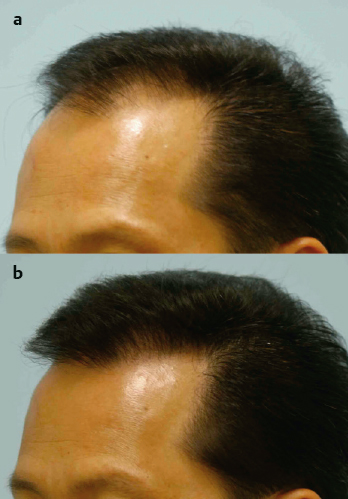
First of all, what is the end objective of performing hair transplant surgery? I would like to state that goal at the outset, which is to provide a strong aesthetic frame to the upper face. Similarly, fat grafting around the eyes can help with providing an eye frame, filling the temple and outer cheek can provide an outer facial frame, and facelifting/chin implants/volumization can provide a lower face frame. When the hairline has been re-established for either a man or a woman, the face looks more attractive and youthful instantly. The frame of the upper face is comprised of two components: the central hairline and the temple hairline. Not every person needs both horizontal (central) and vertical (temple) hairlines improved, but it is worthwhile for the reader to understand the importance of considering these options (Fig. 23.2).
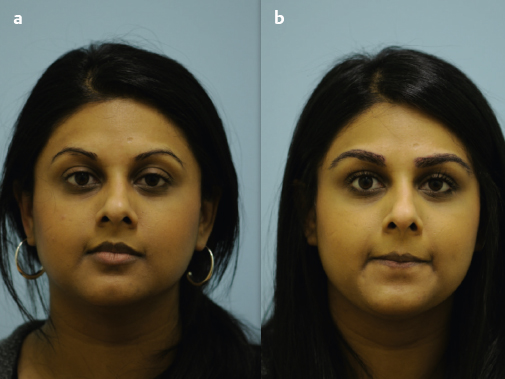
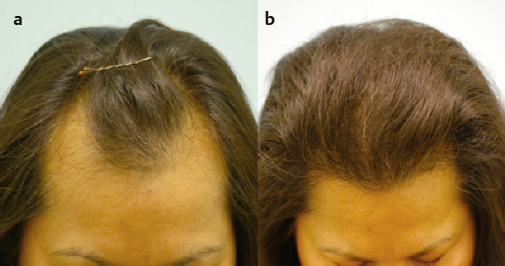
Other examples of facial framing with hair restoration include an eyebrow hair transplant (Fig. 23.3) that will frame the eye, and a crown hair transplant (Fig. 23.4) that will frame the back of the head. All of these elements can provide improvement for the Asian patient. Even women lose their facial frame and can benefit from hair restoration as part of a global strategy of rejuvenation (Fig. 23.5).

Today, hair transplant surgery can produce results as incredibly natural as any other type of facial procedure. Many surgeons still recall the unnatural appearance of plug grafts that transformed a patient into a doll’s head. However, no longer is that the case. Using naturally occurring clusters of hair known as follicular units, transplants can be performed and bring incredible naturalness. What gives me absolute pleasure in working with hair transplantation is the artistry that can be exercised during any procedure, from designing a hairline or eyebrow to allocating grafts with the density gradient that is optimal for a particular patient. The tedium that many surgeons associate with the surgical procedure lies in their ignorance of how much enjoyment can be had when performing it.
The Asian patient has a few very salient differences from other races that should be considered before performing a procedure on him or her. First, the hairs typically are very dark, very coarse, and very straight and are set against a paler to moderately dark skin. This is perhaps the worst combination of characteristics to have when one wants to achieve naturalness. The darker, coarser, and straighter hair, especially when set against a scalp that is fairer in complexion, can make a graft look unnatural if not perfectly executed. It is, however, extremely easy for the technician team to dissect and transplant these grafts because they are so dark, coarse, and straight. The surgical team must take steps to ensure that the result appears absolutely natural in every way. To ensure this outcome, I almost always perform an increased number of singlehair grafts along the frontal hairline so that the hairline looks natural. For example, I may use only 150 to 200 singlehair grafts in a light-skinned, light-colored, fine- and curly-haired individual. In contrast, I may use twice that number of singlehair grafts for an Asian patient before I even contemplate starting with twohair grafts because I want the hairline to appear very soft in nature. The recipient sites that are made to accommodate these grafts form what is known as the “micro” hairline. The “macro” hairline refers to the actual initial line drawn on the scalp into which these recipient sites will be placed. The macro hairline drawn on the typical Asian also can look quite different from that in the Caucasian patient. The macro hairline is typically rounder in shape with less suppression or concavity along the lateral extent of the hairline, which matches the rounder shape of many Asian faces. A very narrow hairline often will not look quite right on an Asian patient because the hairline shape will not match the face or will not match a hairline that exists in this race. Studying natural, nonbalding hairlines in Asians can be a good guide to training one’s aesthetic eye with real-world examples before beginning to operate on these individuals.
There are two types of donor harvesting that are currently offered. The traditional method of graft harvesting is known as follicular unit transplant, or FUT, which involves a linear strip from the back of the head. The newer method, which involves small punches and avoids the linear incision, is known as follicular unit extraction, or FUE. FUT still plays a very significant role for many of my patients for several reasons. First, grafts that are taken through a linear harvest and then dissected are unquestionably healthier and thereby have an increased survival rate after transplantation. Even the very best FUE grafts are more fragile and, even with the most assiduous handling and transplantation of them, are still less viable relative to FUT. Second, FUE may not be the best way to optimize the use of the donor hair region, in that grafts must be taken very broadly across the entire expanse of the back of the head, and that may cause several problems. First, there can be donor depletion if you take more than 20% of the grafts, leading to a moth-eaten appearance or diminished density in the donor area. Second, FUE is not a scarless procedure and can lead to punctate white dots correlating with where the punches have taken the grafts. Third, because harvesting must occur in a wide expanse, the harvest can approach or exceed the defined safe donor area; that is, future hair loss can progress into the areas where harvesting occurred, leading to loss of transplanted grafts in a haphazard fashion. FUE scars are more visible as well in patients with greater pigmentation since the scars are typically hypopigmented in nature. FUT, however, is not without risk either, particularly in the Asian. Because Asians tend to create more exuberant scar formation than Caucasians, at times a thicker scar may develop in the donor area. Further, because the donor hair is very dark black and very straight, the white line of a scar can be more visible than in many other races. These considerations are meant to serve only as guidelines for a physician who is interested in performing a hair transplant in an Asian patient, and are not intended to frighten or mislead either a prospective surgeon or patient.
Recently, there has been a rise in the use of regenerative medicine techniques that I like to refer to as “fertilizers” since these adjunctive measures help transplanted hairs grow much better, faster, and more consistently. The donor scar can be helped with these products as well. The three major products that we use are MatriStem (ACell), plateletrich plasma (PRP), and adenosine triphosphate (ATP). It lies beyond the scope of this chapter to discuss how and why each of these products is used. Suffice it to say that I believe these products are indispensable for every hair transplant procedure that I perform and can be very helpful to achieve better outcomes whether the patient is Asian or not.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


