24 Facial Fat Grafting
Pearls
Reducing the initial excessive expectations of the patient by adequate counseling is important.
The structural and functional relationship of the aging and soft tissue foundations under the influence of gravity should be considered to avoid an unnatural facial contour after fat grafting.
Fat grafting achieves volumetric lifting by strengthening soft tissue foundations and restoring volume deficiency.
Common fat harvesting sites are the abdomen and lateral thigh, followed by the medial thigh and flank.
Fat grafting of the face should be performed sequentially from the posterosuperior to the antero-inferior area and from the deep layer to the superficial layer.
Pressing or massaging after fat injection must be avoided since it can damage mature adipocytes.
Using an ideal grip technique is important in increasing survival and reducing the complications of fat grafting.
Fat injections must always be performed as the syringe or cannula is being drawn back to prevent vascular occlusion.
When injecting fat into the forehead area, the surgeon is strongly recommended to inject botulinum toxin before the procedure for better fat survival, with the exception of patients who have eyelid ptosis.
Fat injection is not a procedure without complications. Serious complications such as infection and vascular occlusion always need both the surgeon’s and the patient’s attention.
Introduction
Autologous fat transfer has been widely used to improve wrinkles, folds, and depressions caused by aging and to treat partial congenital facial hypoplasia. In 2000, Fournier introduced a lipo-filling technique as a good solution for reversing the aging process via volume surgery. Also, he was the first user of the syringe-needle unit or syringe-cannula unit to completely block contact with air.1 Since then, complementary fat grafting has been frequently used as an adjunctive treatment to restore volume deficiency that cannot be improved by conventional rhytidectomy.2
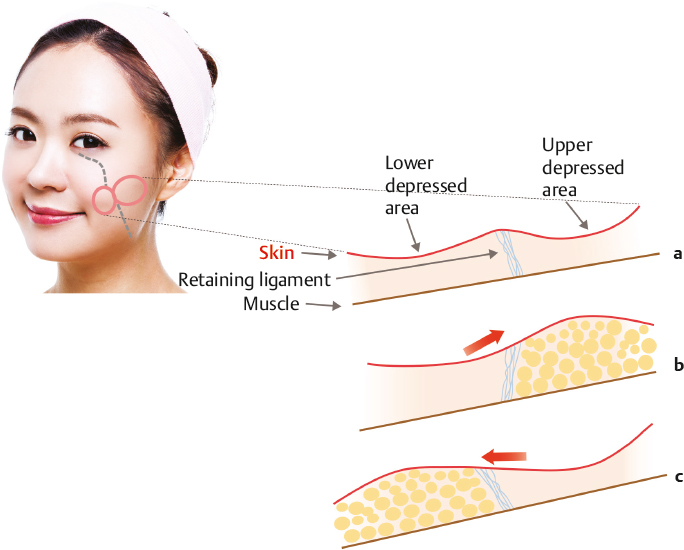
At present, fat grafting is done not only for volume recovery, but for facial contour improvement as well. Despite the surgeon’s attempts to achieve successful fat grafting, an unnatural facial contour such as a flat, broad, and sagged appearance can occur when the fat is injected only for the correction of volume depletion, with no consideration of the structural and functional relationship of the aging and soft tissue foundations.3 Special structures that maintain soft tissue contours by restricting or fixing the movement of facial soft tissue are classified according to three morphologic forms: retaining ligament, septum, and adhesion. However, with aging as well as after years of muscular activities and the pull of gravity, the ligamentous fixations become distended, elongated, and thinned due to the decrease of collagen fiber and loss of intra- and peri-ligamental fat. Eventually, the soft tissue foundations become weak and laxity of face ensues. Autologous fat can be injected into the intra- and peri-ligamental space, thereby strengthening the attenuated ligamentous fixation to provide solid soft tissue foundations.
Thus, to achieve a successful outcome in fat injection, a systematic approach considering the roles of various structures related to facial contour, the structural changes imposed by the aging process, and the influence of gravity is necessary. Considering all these factors, the whole face is divided into several zones, and the autologous fat is grafted according to a specific sequence of injections.
Patient Evaluation
The physician should evaluate the facial proportions, degree of aging, and the facial shape of the patient (oval, round, heart, square, rectangle, inverted triangle, triangle, and diamond shapes). According to the facial shape and degree of aging, the physician can recommend the best approach for fat grafting that can make the patient’s face look younger, smaller, and more beautiful. For example, fat grafting for anterior projection is recommended in a broad and flat face. Volumetric lifting using fat grafting is recommended in a sagged, triangular, or rectangular face. An asymmetric face or facial expression should be evaluated prior to the procedure. According to the degree of asymmetry, the amount of fat and level of placement should differ.
To predict the total amount of fat to be injected, it is necessary to identify the areas where the patient wants grafting, and to confirm other areas necessary to create natural contour without sagging, even if the patient does not want to perform fat grafting in those areas. Additionally, the thickness and elasticity of the skin and subcutaneous tissue should be checked to adjust the amount of fat and level of placement.
During the consultation, the importance of environmental factors that can decrease the survival rate and longevity of grafted fat should be explained to the patient. The physician must precisely check the patient’s surgical history, including all facelifting procedures, previous fat grafting, allograft implantation, and any injections of artificial fillers including foreign bodies (silicone or paraffin). Other checking points include the hemorrhagic tendencies of currently taken drugs, health foods, and nutritional supplements, such as aspirin, ibuprofen, deer antler, red ginseng, licorice, ephedra, garlic, onion liquid, vitamin E (α-tocopherol), and omega-3 fatty acids. Smoking and drinking should be stopped 1 or 2 weeks prior to the procedure and at least 2 weeks to a maximum of 3 months after the procedure because they increase the incidence of hemorrhage, edema, inflammation, and delayed wound healing. Generally, the turnover of grafted fat occurs within 2 to 3 months after the procedure due to transient reperfusion ischemia, but it can occur after up to 6 months.4 Therefore, it would be good to maintain the patient’s body weight until 6 months after the procedure. It is advisable to inform the patient in advance that if there is a need for additional fat grafting, it should be done within 3 months after the first procedure, as such timing is safer and is associated with better effects. When the patient has asymmetric facial movement, botulinum toxin can be injected 2 weeks prior to the planned procedure.
Because facial fat grafting brings dramatic changes in facial appearance as time passes, pre- and postoperative photographing is very important to evaluate the effects. A sky-blue background is preferred because skin color is expressed better and it can have shadow thinning effects. A strobe flash is a good light source since it is close to natural light. Use of a standard lens that has a 50-mm distance between the camera and the lens is recommended.
Procedural Techniques
Instruments and Solutions
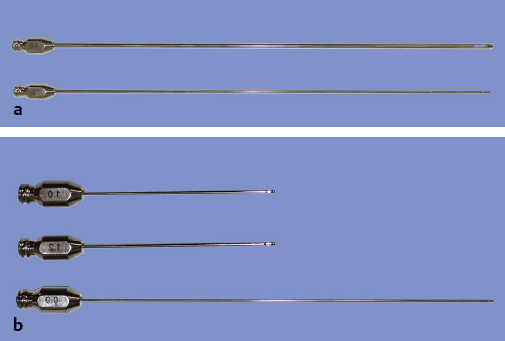
Instruments for harvesting fat include a tumescent infiltrator (1.8 mm [diameter] × 25.0 cm [length]), standard suction cannula (3.0 mm × 25.0 cm), and syringe (Luer lock disposable syringe, 10.0 mL). Instruments for fat injection include a tumescent infiltrator (0.9 mm × 15.0 cm), injection cannula (Coleman Type I, Mentor, 1.2 mm × 7.0 cm; Type II, 1.0 mm × 7.0 cm), and syringe (Luer slip disposable syringe, 1.0 mL) (Fig. 24.1).
For local injection, lidocaine (1,000 mg/L) containing epinephrine (1.0 mg/L) is mixed with bicarbonate (10 mEq/L). Modified Klein solutions for donor and recipient sites are as follows: lidocaine (2,400 mg/L) containing epinephrine (2.0 mg/L) is mixed with bicarbonate (15 mEq/L).
Anesthesia
For fat grafting, local anesthesia combined with oral preoperative medications (cephalexin, acetaminophen, and diazepam) or intravascular sedation (propofol) is usually applied. The author prefers to do fat grafting under sedation, but general anesthesia can also be applied according to the demand of the patient and the anesthetic physician’s requirement according to the medical status of the patient. A nonsteroidal, longlasting antiinflammatory drug such as diclofenac sodium can be given before surgery for preemptive analgesia.
Preparation of Fat for Injection
Liposuction
In donor site selection, the first preference is the abdomen and lateral thigh. The second is the medial thigh and flank. The third is the supra-pubic, anterior thigh, and supra-knee region. However, any body area that is possible for liposuction can be a donor site for fat grafting.
For harvesting fat, the entry site is anesthetized by modified Klein solution for regional anesthesia using an infiltrator attached to a 10-mL Luer lock syringe, and a 3- to 4-mm-long incision is made at the entry site with a surgical blade. The appropriate infiltrated volume of tumescent solution is in a ratio of 1 to 2 mL for each 1 mL of the expected fat harvest.5 A standard suction cannula connected to a Luer lock syringe is introduced for manual liposuction. For this procedure, the plunger of the syringe should be gently handled to provide ~ 1 or 2 mL of negative pressure space in the barrel of the syringe while the cannula is pushed through the harvest site. A high vacuum (more than 2 mL) may damage fat cells during the procedure. The application of skin protector or the patient’s own oil from the fat aspirates to the incision site is helpful in preventing friction burn and hypertrophic scar. All incision sites should be closed with nylon 6.0 interrupted sutures.
Separation of Aspirates
After harvesting, the fat aspirate is centrifuged at 1,200 g for 3 minutes.6 Free oil should be removed by holding the syringe diagonally and pouring the oil out. The contaminated portion can be absorbed or wiped by moist gauze with sterile saline. After eliminating the free oil, the lower fraction, which contains blood and tumescent solution, is discharged and the purified fat is then transferred from the 10-mL Luer lock syringe to a 1.0-mL disposable syringe (Fig. 24.2).

Fat Injection
Regional infiltration of anesthesia with a 1% lidocaine with epinephrine (1:100,000) mixture is injected into the entry site of fat injection for sensory nerve block. The supraorbital, supratrochlear, infraorbital, mental, buccal, zygomaticotemporal, zygomaticofacial, greater auricular, and auriculotemporal nerves are targets of sensory nerve block. Tumescent infiltration can be used for prevention of bleeding, pain, and vascular embolization in the temple, orbital, buccal, and pre-auricular area.
To achieve a successful outcome in fat injection, appropriate design and sequential injection are important. The author introduced the sequential autologous fat injection (SAFI) technique, which was developed to apply fat using a systemic approach.
Face (Temporal, Midface, and Lower Face Regions)
For SAFI, four lines divide the lateral face into five zones (Fig. 24.3). Each zone has several areas for fat grafting. The areas numbered 1, 3, 6, 9, 11, 13, 14, 15, 17, 18, 19, and 21 are the areas where most of the patients want fat grafting. The other numbered areas are the sites where the physician should inject fat for providing strong skeletal support, strengthening the soft tissue foundation, and preventing gravitational descent. The placement and injectable volume of each SAFI area are described in Table 24.1 .
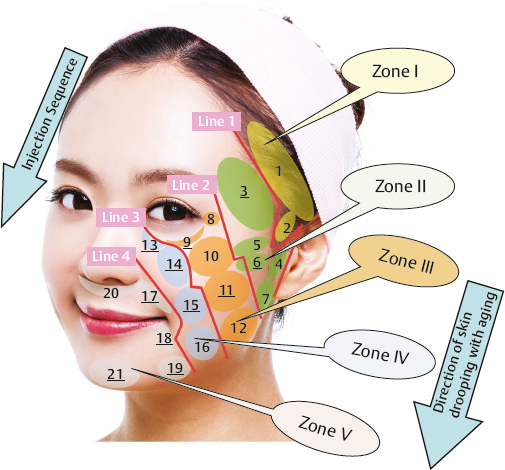
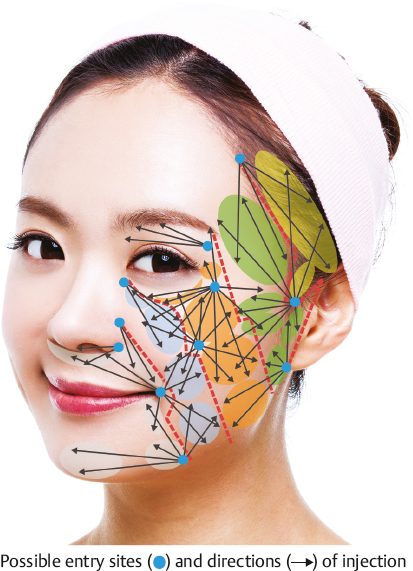
Fig. 24.4 shows the location of entry sites, injectable areas, and advancing directions for the cannula in performing SAFI. The arrows from each entry site indicate the directions and approachable areas for the cannula. However, the selection of the entry sites depends on the status of the patients and the preferred posture or convenience of the physician.
Fat injection is performed in a systematic manner: (1) in the sequence of zones I, II, III, IV, and V; (2) from the posterosuperior area to the antero-inferior area within the same zone (Fig. 24.3); and (3) in the sequence of deep, middle, and superficial layer within an area or its subarea (Fig. 24.5).
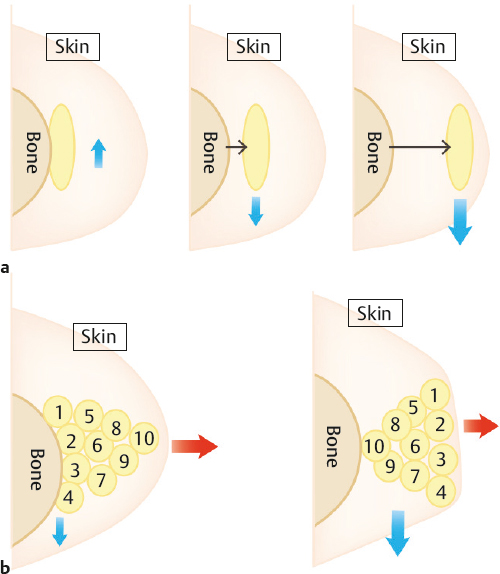
For example, the submalar hollow is divided into two subareas (anterior and lateral) because this area is relatively wide and has a high risk of sagging due to the weak soft tissue foundation. Fat is sequentially injected into the supraperiosteal layer of the zygoma and maxilla for increasing skeletal support, into the masseteric cutaneous ligament for strengthening the soft tissue foundation, and into the atrophied buccal fat pad for increasing fullness (Fig. 24.6).
The nasolabial fold consists of two parts: the lateral bulging caused by volume-depleted pseudo-ptosis and the medial depression caused by the loss of volume. To correct the lateral bulging, fat is injected to the malar, midcheek furrow, and submalar area. To correct the medial depression, injection into the whole layer of the depressed area is necessary.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


