26 Aesthetic Facial Implants
Introduction
Over the last two decades, the marked improvement in biomaterial and the design of facial implants have expanded their use in aesthetic and facial rejuvenation surgery. 1 , 2 , 3 Alloplastic implants offer a longterm solution to augment skeletal deficiency, restore facial contour irregularity, and rejuvenate the midface and mandible. Common implant procedures include cheek augmentation to balance the effects of malar hypoplasia, mandibular augmentation to create a stronger mandibular profile and a better nose–chin relationship, mandibular prejowl and angle implants to augment traditional cervicofacial rhytidectomy, submalar and midfacial implants to augment the hollowness that occurs during the aging process, nasal implants for dorsal augmentation, and premaxillary implants to augment a retrusive midface. Computer-assisted customdesigned implants now provide an improved solution for more complex facial defects in terms of determining the degree of augmentation necessary, and measuring asymmetry over a midsagittal plane for cases due to trauma, congenital deformities, and HIV lipoatrophy. 4 , 5 , 6
The concept of facial contouring implies a change in the shape of the face. The surgeon can produce substantive contour changes by judiciously altering mass and volume in different anatomical regions and redistributing the overlying soft tissue. Accurate facial analysis is critical to the success of using facial implants. The appropriate implant will depend on the relationship between different bony promontories and the surrounding soft tissue. The individual configuration of the nose, malarmidface area, and mandible-jaw line determine the fundamental architectural proportions and contour of the face. Balance between these structures and the constant distribution of the overlying soft tissue structures determines facial beauty and harmony. Modern hallmarks of beauty are distinguished by bold facial contours that are accentuated by youthful convex malarmidface configurations and a sharp, welldefined jaw line. Any of these promontories that are too small or too large affect the aesthetic importance of the others. For example, reducing the nasal prominence causes both the malarmidface and the mandibular-jaw line volume and projection to appear relatively more distinct. In the same manner, enhancement of the mandibular or malarmidface volumes makes the nose appear smaller and less imposing. Typically, when augmentation is the desired goal, it is accomplished through selecting implants with the proper shape and design while controlling their position over the facial skeleton and soft tissue. As a result, alloplastic facial contouring can be utilized to augment bony or soft tissue anomalies.
Implants and Biomaterials
All implant materials induce the formation of fibroconnective tissue encapsulation, which creates a barrier between the host and the implant. 7 , 8 Adverse reactions are a consequence of an unresolved inflammatory response to implant materials. The behavior is also a function of the configuration characteristics of the site of implantation such as the thickness of overlying skin, scarring of the tissue bed, and inherent underlying bone architecture that would tend to create a condition for implant instability. For example, implants that are more deeply placed with thicker overlying soft tissue rarely become exposed or extrude. Other important factors such as prevention of perioperative hematoma, seroma, and infection can significantly reduce host–implant interaction and thereby improve implant survivability. The specific biomaterials currently available include porous polytetrafluoroethylene carbon (Proplast), expanded polytetrafluoroethylene (ePTFE), large-pore high-density polyethylene (Medpor [Stryker]), solid medical-grade silicone rubber (Silastic [Dow Corning]), and polyamide mesh (Supramid [Resorba Wundversorgung]). In addition, composite implants such as ePTFEcoated silicone are commercially available. Porous materials are utilized for their ability to encourage soft tissue ingrowth during the healing process. Nonporous materials such as silicone induce encapsulation without soft tissue ingrowth.
The Ideal Implant
The ideal implant material should be costeffective, nontoxic, nonantigenic, noncarcinogenic, and resistant to infection. It should be inert, easily shaped, conformable, placed effortlessly, permanently maintain its original form, and easily removed if necessary. The implant should be easy to modify, and customize, to the needs of the recipient area during the surgical procedure without compromising the integrity of the implant.
Favorable surface characteristics are important for implant placement and stabilization, and paradoxically equally important to facilitate easy removal and exchangeability without causing injury to surrounding tissues. Implant immobilization is related to their ability to be fixed in place for the lifetime of the patient. The characteristics of implant materials such as silicone elastomer induce the formation of a surrounding capsule that maintains implant position, whereas ePTFE, which encapsulates to a lesser degree, provides fixation with minimal tissue ingrowth. Each material–host interaction provides certain advantages in different clinical settings. Materials that cause significant tissue ingrowth and permanent fixation are often undesirable, particularly if the patient desires to change augmentation characteristics in later years. The natural encapsulation process of silicone and the minimal surface ingrowth in ePTFE products ensure immobility yet provide exchangeability without damage to surrounding soft tissue.
The ideal implant design should have tapered margins that blend onto the adjacent bony surface to create a nonpalpable and smooth transition to the surrounding recipient area. An implant that is malleable and readily conforms to the underlying structures further reduces mobility, while the anterior surface shape should imitate the desired natural anatomical configuration. Newer silicone implants have been engineered for enhanced conformability to the underlying bony surface and surrounding soft tissue. For example, Conform implants (Implantech) with grid backing reduce the memory of the silicone elastomer and improve flexibility. Greater adaptability to irregular bony surfaces reduces chances of movement and prevents posterior dead space from occurring between the implant and underlying bone ( Fig. 26.1 ). Renewed interest in research and development in biomaterial engineering have developed a composite implant (using both silicone and ePTFE) that combines the advantages of two biomaterials for facial implants. 9

Implant Biomaterials
Polymeric Materials/Solid Polymers
Silicone Polymers
Since the 1950s, various forms of silicone have been clinically used with excellent safety efficacy profile. Silicone is polymerized dimethylsiloxane that can be solid, gel, or liquid depending on its polymerization and cross-linkage. Solid silicone products tend to be more stable. The gel form of silicone can potentially over time leak some of its internal molecular substances. However, the most recent studies on breast implant gel silicone have shown no objective cause and effect for silicone in producing scleroderma, lupus, collagen vascular, or other autoimmune diseases. 10 , 11 Solid silicone elastomer has a high degree of chemical inertness. It is hydrophobic and extremely stable without any evidence of toxicity or allergic reactions. 12 Tissue reaction to solid silicone implants is characterized by a fibrous tissue capsule without tissue ingrowth. When unstable or placed without adequate soft tissue coverage, the implants are subject to moderate ongoing inflammation and possible seroma formation. Capsular contracture and implant deformity rarely occurs unless the implant is placed too superficially or if it migrates to the overlying skin.
Polymethacrylate (Acrylic) Polymers
This is supplied as a powdered mixture and catalyzed to produce a very hard material. The rigidity and hardness of the acrylic implants cause difficulty in many of the applications for using large implants inserted through small openings. In the preformed state, there is no ability to adapt the implant to the underlying bony contour surface changes.
Polyethylene
Polyethylene can be produced in a variety of consistencies, now most commonly used in a porous form. Porous polyethylene, also known as Medpor, causes minimal inflammatory cell reaction. The material, however, is hard and difficult to sculpt. The porosity of polyethylene permits extensive fibrous tissue ingrowth that provides an advantage for enhanced implant stability but makes it extremely difficult to remove without damage to surrounding soft tissue, bleeding, and potential injury to adjacent neurovascular bundles.
Polytetrafluoroethylene
Polytetrafluoroethylene is comprised of a group of materials that has had a defined history of clinical application. The known brand name was Proplast, which is no longer made in the United States because of the related complications of its use in temporomandibular joints. Under excessive mechanical stress, this implant material was subject to breakdown, intense inflammation, thick capsule formation, infection, and ultimate extrusion or explantation.
Expanded Polytetrafluoroethylene
ePTFE was originally produced for cardiovascular applications. 13 , 14 Animal studies showed the material to elicit limited fibrous tissue ingrowth without capsule formation and minimum inflammatory cell reaction. The reaction seen over time compared favorably with many of the materials in use for facial augmentation. The material has found acceptable results in subcutaneous tissue augmentation and for use as preformed implants. Due to lack of significant tissue ingrowth, ePTFE offers advantages in subcutaneous tissue augmentation since it can be modified secondarily and removed in the event of infection.
Mesh Polymers
The mesh polymers, which include Marlex (Chevron Phillips), Dacron (INVISTA), and Mersilene (Ethicon), have similar advantages of being able to be folded, sutured, and shaped with relative ease, but also promote fibrous tissue ingrowth causing difficulty with secondary removal. Supramid is a polyamide mesh derivative of nylon that is unstable in vivo. It elicits a mild foreign body reaction with multinucleated giant cells, and over time causes implant degradation and resorption. 15
Metals
Metals consist essentially of stainless steel, Vitallium, gold, and titanium. Except for use of gold in eyelid reanimation and dentistry, titanium has become the metal of choice for longterm implantation. The advantages of titanium include high biocompatibility, corrosion resistance, strength, and minimal X-ray attenuation during computed tomography (CT) scanning or magnetic resonance imaging. Titanium is primarily used in craniofacial reconstruction and has no use in facial augmentation.
Calcium Phosphate
Calcium phosphate or hydroxylapatite materials are not osteoconductive but do provide a substrate into which bone from adjacent areas can be deposited. 16 The granule form of hydroxylapatite crystals are used in oral and maxillofacial surgery for augmenting alveolar ridge. The block form has been used as interpositional grafts in osteotomies. 17 However, they have been shown to be of less value as an augmentation or onlay material due to its brittleness, difficulty in contouring, and inability to adapt to bone surface irregularities and mobility.
Autografts, Homografts, and Xenografts
Autografts, available as autogenous bone, cartilage, and fat, are limited by donor site morbidity and limitation of available donor material. Processed homograft cartilage has been used in nasal reconstruction, but eventually succumbs to resorption, distortion, and fibrosis.
Tissue Engineered Biocompatible Implants
During the past several years, tissue engineering has emerged as an interdisciplinary field. Properties of synthetic compounds are manipulated to enable delivery of an aggregate of dissociated cells into a host in order to re-create new functional tissue. The field of tissue engineering has evolved by combining scientific advances in multiple fields including material science, tissue culture, and transplantation. These techniques facilitate the seeding of cells into a suspension that provides a threedimensional (3D) environment that promotes matrix formation. This structure anchors cells and permits nutrition and gas exchange with the ultimate formation of new tissue in the shape of a gelatinous material. 18 A number of tissue engineered cartilage implants have previously been generated based upon these new principles. This includes joint articular cartilage, tracheal rings, and auricular constructs. Tissue engineering offers the potential to grow cartilage in a precisely predetermined shape, and presently is in the developmental stage of generating various types of contoured facial implants consisting of immunocompatible cells and matrix. 19 Once employed on a commercial basis, these techniques would require minimal donor site morbidity and, like alloplastic implants, reduce operative time.
Surgical Considerations for Alloplastic Implants
Patients endowed with strong, well-balanced skeletal features will best endure the negative effects of aging. 20 Analysis of the faces of teens reveals an abundance of soft tissue that provides the underlying framework for the harmonious composite of youthful facial form. Full cheeks with smooth, symmetrical contours and free of sharp, irregular projections, indentations, rhytids, or dyschromias commonly embody these youthful qualities. 21 Facial aging is influenced by genetic factors, sun exposure, smoking, underlying diseases, gravity, and the effects of muscular action upon the overlying soft tissue and the underlying bone which produces hyperfunctional lines of aging and bone resorption. 22 , 23
Depending on the underlying skeletal structure, involutional soft tissue changes associated with the aging process bring about definable configurations of the face that appear progressively more obvious and pronounced with time. Recognizing these various defects and configurations is an integral part of determining if a patient is a candidate for facial contouring procedures. Facial involutional changes contribute to the flattening of the midface, thinning of the vermillion border of the lips, development of deep cavitary depressions in the cheek, and formation of deep skin folds and rhytides. 24 Other specific soft tissue configurations include the prominence of the nasolabial folds, flattening of the soft tissue button of the chin, and formation of the prejowl sulcus ( Fig. 26.2 ). 1 , 25
It has been well established that facial skeleton changes also occur during the aging process. The volume loss and resulting loss of facial architecture must be addressed to restore a robust skeletal framework in order to properly drape the augmented soft tissue envelope for a more youthful appearance. Skeletal changes include resorption of the mandible and maxilla that result in changes such as an increased orbital aperture and loss of mandibular height and length. 22 For patients with adequate soft tissue volume, restoration of skeletal volume deficiencies such as midface, prejowl, and gonial angles can provide a more youthful appearance without an accompanying soft tissue procedure ( Fig. 26.3 ).

The ability to permanently replace soft tissue volume in sufficient quantity is one of the most elusive aspects of facial rejuvenation. The recent popularity of fat transplantation has reemphasized tissue replacement as a key component of the rejuvenation process. Alloplastic augmentation techniques are able to permanently address these problems by softening sharp angles or depressions, re-expanding the underlying surface to reduce rhytids, as well as enhance inadequate skeletal structure. 26 , 27 , 28
Nasal and Premaxillary Augmentation
The relatively thin skin overlying the nasal dorsum often fails to provide adequate camouflage for poorly contoured replacement tissue. Nasal augmentation has been performed using many different materials. Effective longterm dorsal nasal reconstruction has continued to remain problematic despite extensive efforts to use a wide variety of autografts, allografts, and alloplastic materials. A suitable replacement implant to reconstruct the original nasal profile must possess a number of unique characteristics. Its shape must be of adequate length and have consistent curves, thickness, and tapered edges so that it can fit well over the nasal bridge and blend in with the surrounding soft tissues and bone. It must also possess a high degree of malleability, flexibility, and compliance so that the implant can endure longterm stress and trauma.
Autogenous tissues such as calvarial bone grafts as well as septal, conchal, and costal cartilage are always preferred. However, septal and conchal cartilages often do not provide adequate volume. Costal cartilage and calvarial bone grafts have additional donor site morbidity. Costal cartilage also has the potential to warp if not carved properly. Homograft cartilage has also been utilized for nasal reconstruction but has a high percentage of resorption. Currently, the most commonly used alloplastic implants for nasal augmentation consist of silicone, ePTFE, and polyethylene (Medpor). Silicone can eventually produce overlying skin atrophy and must be anchored to prevent movement. Also, silicone and ePTFE have the potential for infection, but are easily removed and replaced. Polyethylene implants (Medpor), as with any other implant that promotes significant tissue ingrowth, has the potential for major soft tissue damage to the overlying skin if removal becomes necessary. In addition, rigid implants have a high extrusion rate when implanted in regions with soft tissue mobility such as the columella and alar side walls due to nasalis muscle contracture. 29 , 30
The use of autogenous tissue avoids the problem of incompatibility, but sometimes fails to provide necessary volume to provide the size and shape. A more ideal substitute to replace deficient skeletal structure, particularly over the nasal dorsum, would be a neocartilage graft reproduced from one’s own cells that closely mimics the original skeletal contour. This cartilage implant can be synthesized through the process of tissue engineering. 31 The concept involves use of donor septal cartilaginous tissue which is harvested and then broken down into its cellular components. The cells are cultured in vitro, permitting them to multiply. A synthetic alginate scaffold is created in the shape of a dorsal nasal implant through a molding process. The cells are impregnated into the gelatin scaffold, which is placed subcutaneously into mice and permitted to evolve, in vivo, into a final shape. It is during this phase that the alginate scaffold slowly dissolves and is replaced by viable hyaline cartilage. The cartilage is then harvested as an autogenous implant. This process has the potential of becoming a valuable addition to nasal and facial augmentation in the near future. 32
An often overlooked area in facial analysis, particularly in rhinoplasty, includes the premaxillary region. Proper evaluation and augmentation techniques can improve facial contour principally in the midline. Premaxillary deficiency is very common in the Asian population; however, premaxillary deficiency often goes unnoticed in the general population. Deficiency inferior to the nasal spine region results in a retrusive maxilla and the appearance of a shortened upper lip/philtrum complex. Augmentation of this region addresses many aesthetic shortcomings such as increasing nasal projection, improving the nasolabial angle, and lengthening of the upper lip. 33 Autogenous or alloplastic grafts can typically be inserted through an intranasal inferiorly based hemitransfixion incision by elevating the periosteum of the premaxilla and creating an adequate pocket for implantation. In most cases, it is not enough to only augment the nasal spine. Rather, the entire premaxilla extending laterally to the peripyriform aperture must be augmented.
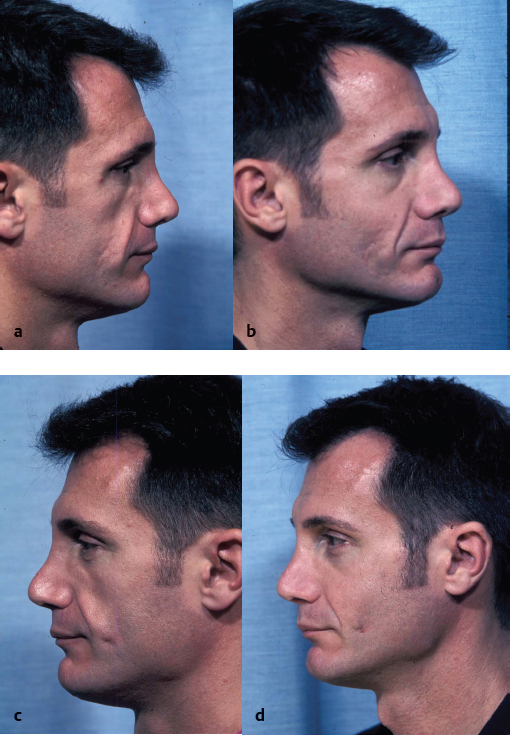
Alloplastic implantation techniques for premaxillary augmentation include autologous cartilage, prefabricated silicone implants, and rolled sheets of ePTFE that are fashioned to augment the region inferior to the nasal spine. These are easily inserted via a hemitransfixion incision, and secured to the periosteum, providing a relatively simple solution for this aesthetic deficiency. This improves an acute nasolabial angle and augments the midface, resulting in a pleasing midface contour with a more pronounced nasal projection. Rolled sheeting of ePTFE has the advantage of conforming to the underlying bone and can be fixated to the nasal spine without the deficit in smile due to soft tissue impingement. There is minimal movement of the implanted material leading to a decreased risk of implant extrusion ( Fig. 26.4 ).

Midface Augmentation
Rhytidectomy has become just one component of facial rejuvenation. Midfacial augmentation, midface lifts, and resurfacing techniques all must be considered when customizing a surgical plan for the patient. The pathophysiology of the aging process is a key factor in determining the correct surgical treatment. It is now well understood that the aging process not only results in the descent of the midface but also in the atrophy of the soft tissue in multiple facial planes. Midface rejuvenation can therefore be achieved not only through suspension techniques, but also by the augmentation of the soft tissue and skeletal foundation. Alloplastic augmentation is an effective way to alter the midface appearance in appropriate candidates. Midface augmentation is a straightforward, longlasting, and relatively low risk surgical option that can consistently and predictably improve midface aesthetics. It has the ability to not only replace lost facial soft tissue volume but also increase the anterolateral projection of the area thereby improving midface laxity and decreasing the depth of the nasolabial folds. Implants are readily reversible and can be combined with standard rhytidectomy procedures. The net effect is softening of the sharp angles and depressions of the aged face resulting in a natural “unoperated” look. In appropriate candidates, moderate facial rejuvenation can be achieved simply with the placement of submalar midface implants without concomitant rhytidectomy.
Midface augmentation can also facilitate rhytidectomy in several ways. The skin and soft tissue can be draped over a broader, more convex midface region after implant augmentation. There is also minimal traction on the perioral tissues and lateral commissure if placed prior to the rhytidectomy, which can help to avoid an “over-pulled” appearance. Finally, release of the underlying osteocutaneous ligaments at the zygoma and mandible allow for an improved ability to vertically lift the soft tissue which further avoids an unflattering result. Many patients who present for revision rhytidectomy that require volume restoration can also be improved by expanding the midface region, while decreasing downward vertical traction forces on the lower eyelid.
Specific criteria are available for determining regions of aesthetic deficits and their corresponding alloplastic solutions. 34 , 35 In addition, other regions that contribute to the midfacial appearance must be carefully considered during patient evaluation. In the periorbital region, the aging process results in the weakening of the orbital septum and herniation of the periorbital fat, causing infraorbital bulges. The orbicularis muscle becomes ptotic, especially in its most inferior aspect. The use of conventional blepharoplasty will tend to exacerbate laxity of the lower canthal ligament which can contribute to the formation of the tear trough deformity and lower lid malposition. 36 , 37 Attendant with aging is subcutaneous tissue atrophy which has more damaging effects on the very thin infraorbital skin accounting for the hollowness of the eyes with advanced aging. Skeletal insufficiency and imbalances are usually caused primarily by the hypoplastic development and inherent bony imbalances of the facial skeleton that are exacerbated by the aging process. Midfacial descent involves ptosis of the infraorbital subcutaneous tissues, malar fat pad, suborbicularis oculi fat (SOOF), and orbicularis muscle. As the cheek falls and collects on the upper nasolabial fold, the thicker tissues of the malar fat pad descend and leave the infraorbital region exposed to thin soft tissue covering. Thus the nasojugal/tear trough region becomes prominent, lower eyes appear hollow, and infraorbital rim becomes more prominent. The loss of subcutaneous tissues occurs throughout the body, but in particular affects midfacial tissues more severely, including the buccal fat pad, the malar fat pad, and the SOOF. As these tissues continue to lose volume and descend, different patterns of midfacial aging develop in the infraorbital and cheek regions.
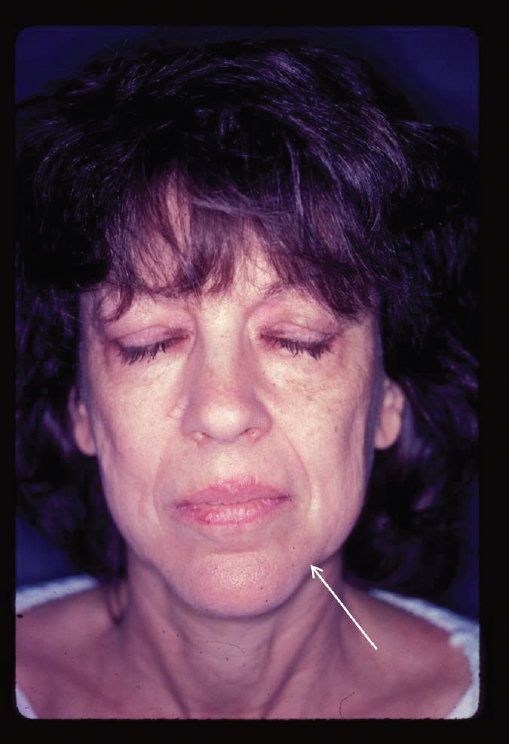
In the midface, most soft tissue deficiencies are found within the recess described as the submalar triangle. 38 This inverted triangular area of midfacial depression is bordered above by the prominence of the zygoma, medially by the nasolabial fold, and laterally by the body of the masseter muscle ( Fig. 26.5 ). The aging process is exaggerated when severe soft tissue involutional changes are associated with deficient underlying bone structure. Facial depressions can also become apparent in individuals who have prominent cheek bones combined with thin skin lacking subcutaneous or deep supporting fat. This type of pattern causes a gaunt appearance in an otherwise healthy person. The severe form of this midfacial pattern can be seen in anorexia nervosa, starvation, or in HIVassociated lipoatrophy. In combination with the primary disease process, protease inhibitors and other newer generation HIV therapies have a predilection for erosion of the midfacial fat and the buccal fat pad ( Fig. 26.6 ). 4 , 5 These conditions of volume loss that are also associated with the aging process often preclude rhytidectomy, alone, to completely rejuvenate the face and are currently being successfully treated with the use of computerassisted customdesigned facial implants. 6

For successful rejuvenation of the midface, a 3D approach must be utilized. The descent and volume loss of the midface must be camouflaged, corrected, or replaced. The surgeon must therefore approach facial rejuvenation using a multilevel as well as a multimodality method. Camouflage techniques such as lower blepharoplasty with fat repositioning can result in the blunting of the nasojugal groove/tear trough region by securing the infraorbital fat past the arcus marginalis. 39 Alloplastic or autogenous augmentation techniques reverse the effects of midfacial descent by replacing midfacial volume loss and providing soft tissue support at the deepest plane. These adjunctive procedures can also be performed with rhytidectomy procedures for an improved and prolonged aesthetic result. Acknowledging the many elements of structural deficiency and phenomena of aging, multimodality treatments are necessary to restore the face to a more youthful appearance. 40
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


