25 The Management of Eyelid, Orbital, and Lacrimal Trauma
Abstract
“The Management of Eyelid, Orbital, and Lacrimal Trauma” discusses this topic for ophthalmologists who, regardless of the type of practice they have, may be called upon to manage patients who have sustained acute eyelid, lacrimal, or orbital trauma. A systematic approach to the evaluation and management of such patients by the ophthalmologist is essential to maximize the results of primary treatment; minimize the need for secondary reconstruction; avoid the risk of missing serious sight- or life-threatening injuries; and lessen the exposure of the ophthalmologist to medicolegal risks. Cardinal principles are to examine and treat the patient for all injuries; maintain a high index of suspicion for undetected injury; determine the priority for repair; delay major reconstruction if the necessary expertise is not available; delay the repair until operating conditions are optimal; document all injuries very carefully; remove dirt and debris; reposition tissues to their correct anatomical alignment; and do not discard or excise tissue unnecessarily. Most patients who suffer acute eyelid, lacrimal, or orbital trauma present to a general emergency department, where the initial diagnosis is made. Eyelid trauma that is apparently trivial may be associated with serious sight-threatening or even life-threatening injury that may go undetected. For example, lacerations of the eyelid must be considered to have an underlying perforating injury of the eyeball or even a penetrating injury of the brain until proven otherwise.
25.1 Introduction
Many ophthalmologists, regardless of the type of practice they have, may be called upon to assist in the management of patients who have sustained acute eyelid, lacrimal, or orbital trauma. A systematic approach to the evaluation and management of such patients by the ophthalmologist is essential to do the following:
Maximize the results of primary treatment.
Minimize the need for secondary reconstruction.
Avoid the risk of missing serious sight- or life-threatening injuries.
Lessen the exposure of the ophthalmologist to medicolegal risks.
When called upon to manage a patient who has sustained acute eyelid, lacrimal, or orbital trauma, it is useful to apply a set of cardinal principles (Box 25.1).
Box 25.1 Cardinal Principles
Examine and treat the patient for all injuries.
Maintain a high index of suspicion for undetected injury.
Determine the priority for repair.
The results of primary repair are superior to those of secondary repair.
Delay major reconstruction if the necessary expertise is not available.
Delay the repair until operating conditions are optimal.
Document all injuries very carefully.
Remove dirt and debris.
Reposition tissues to their correct anatomical alignment.
Do not discard or excise tissue unnecessarily.
Most patients who suffer acute eyelid, lacrimal, or orbital trauma present to a general emergency department. There, initial triage and stabilization begin. Although the diagnosis of associated injuries is usually made independently of the ophthalmologist’s examination, a certain redundancy in evaluation is necessary for trauma to be treated appropriately and expeditiously.
Key Point
It is imperative that the patient is examined thoroughly so that additional injuries are not overlooked. The ophthalmologist should assist other specialists in determining the priority for repair of the patient’s injuries.
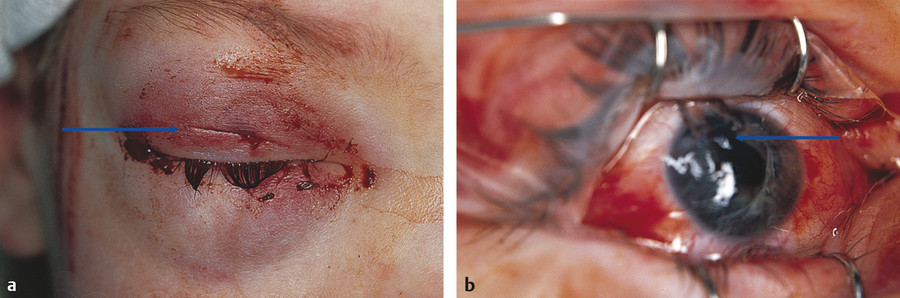
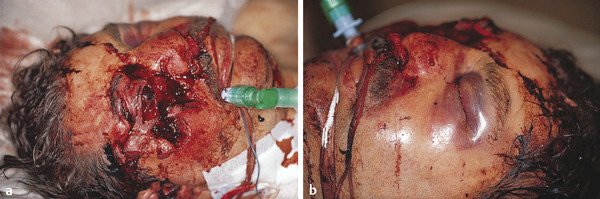
Examine and treat the patient for all injuries (Fig. 25‑1 and Fig. 25‑2).
25.2 History
25.2.1 Mechanism of Injury
Even before seeing the patient, the ophthalmologist can anticipate the types of injuries that are most likely to be encountered from a knowledge of the mechanism of injury. An accurate history is essential, but in many instances, the history may be inaccurate (e.g., self-inflicted trauma, a child whose injury was not witnessed).
Key Point
Apparently trivial eyelid trauma may be associated with serious sight-threatening or even life-threatening injury, which will go undetected unless a high index of suspicion is maintained during the patient’s evaluation.
The examination of patients who have sustained eyelid and/or orbital trauma should be performed very delicately and meticulously to exclude associated trauma to the globe (Fig. 25‑1).
Key Point
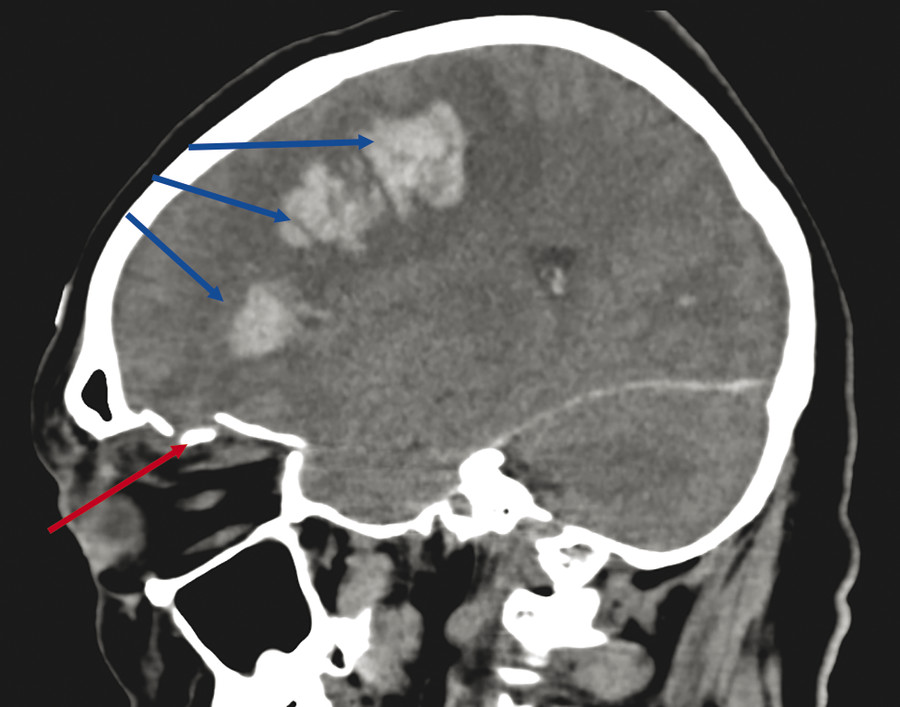
Lacerations of the eyelid have an underlying perforating injury of the globe, or even a penetrating injury of the brain, until proven otherwise (Fig. 25‑2).
Key Point
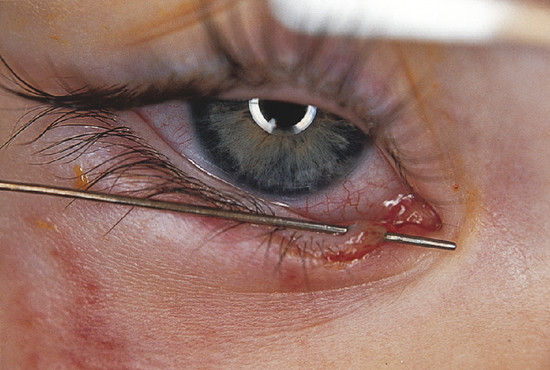
Lacerations of the medial canthal area involve the lacrimal drainage apparatus until proven otherwise (Fig. 25‑3).
Maintain a high index of suspicion for undetected injury.
Eyelid and orbital injuries occur after contact with sharp or blunt objects, toxic substances, or sources of thermal or electromagnetic energy. Combination injuries may be present, such as those seen in road traffic accidents.
25.2.2 Sharp Trauma
Sharp trauma tends to produce a clean wound to the eyelids without actual tissue loss. Sharp trauma can be associated with ocular injury, injury to extraocular muscles or other orbital structures or through penetration of the orbital walls, or craniocerebral or upper respiratory tract injuries.
Key Point
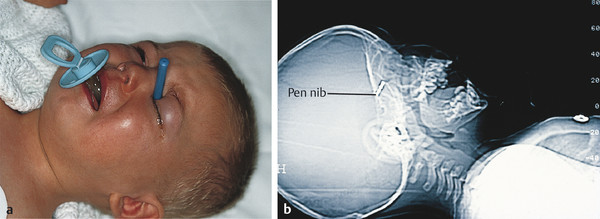
The ophthalmologist must maintain a high index of suspicion for undetected injury and for retained foreign bodies, especially in young children whose injury has not been witnessed (Fig. 25‑4).
25.2.3 Blunt Trauma
Abrasions, irregular lacerations, and partial avulsions are more common with blunt trauma than with sharp trauma. Associated neurological injury (intracranial or cervical), facial fractures, orbital wall blowout fractures, concussive ocular injury, or globe rupture must be ruled out.
Key Point
Computed tomography (CT) should be performed whenever there is clinical evidence of orbital trauma or the suspicion of an intraorbital foreign body.
25.2.4 Bites
Eyelid injuries caused by bites pose unique problems. The injuries themselves can be a combination of sharp and blunt trauma, causing lacerations and tearing-type injuries and, rarely, actual tissue loss. Most periorbital bites are caused by domestic dogs (Fig. 25‑5). Facial and eyelid bites from other animals are extremely rare. Periorbital human bites are also rare but potentially serious.

Key Point
All bite wounds should be considered contaminated, and preventive measures must be taken against possible infection.
25.3 Patient Evaluation
Eyelid trauma is highly visible and, in most cases, alarming in appearance to the patient. Anxiety about the possibility of loss of vision and disfigurement is high and must be managed tactfully. Patients who are under the influence of drugs or alcohol are often particularly difficult to evaluate satisfactorily. Steps should be taken to prevent further inadvertent injury.
Key Point
It should be borne in mind that legal actions often result from the injury, and possibly from the treatment, if the results are unsatisfactory.
25.3.1 Systemic Considerations
The ophthalmologist may be working alone in the case of a patient who has sustained an eyelid laceration and a penetrating eye injury, or he or she may be part of a multidisciplinary team managing a severely traumatized patient, such as after a road traffic accident. After life-threatening associated injuries have been ruled out, acute sight-threatening conditions must be assessed.
Determine the priority for repair.
The patient’s injuries must be dealt with in their order of importance and severity. It is obvious to an ophthalmologist that the repair of a penetrating injury takes precedence over the repair of eyelid lacerations. It may not be obvious to another team, however, that the immediate management of a sight-threatening orbital hematoma takes precedence over visually dramatic facial lacerations once hemostasis has been obtained (Fig. 25‑6). The evaluation of an unconscious patient is particularly difficult. The ophthalmologist plays a very important role in such a situation when the proper evaluation of a relative afferent pupil defect cannot be delegated to other clinicians.
Resuscitation, if needed, and stabilization of vital signs are the initial goals for the treatment of any trauma patient. It must be borne in mind that any patient who has sustained trauma has the potential to develop shock during the evaluation process as a result of occult serious or life-threatening injury. Periodic monitoring of vital signs during the examination process is therefore mandatory. Once the patient has been stabilized, the presence of life-threatening associated injury must be ruled out. Understanding the mechanism of injury is most helpful in this regard (e.g., an eyelid injury from a screwdriver in a child or a fall onto a bamboo cane in the garden in an older individual may be associated with a serious central nervous system [CNS] injury [see Fig. 25‑2]).
All patients with significant eyelid trauma should receive a complete ophthalmic examination, but the order and venue for the examination (in the emergency department or the operating room) are dictated by the severity of associated ocular injury. It is important to ensure that all steps have been taken to exclude possible associated trauma (e.g., CNS injury in a patient with an upper lid puncture wound) by CT before the patient is anesthetized. It is highly unsatisfactory to discover other injuries that require the expertise of other specialists or operating facilities that are located elsewhere once the patient has been anesthetized.
In patients with animal bites it is important to establish whether the patient is immunocompromised and, in particular, whether a prior splenectomy has been performed, so that the increased risk of possible posttraumatic infection with unusual organisms can be assessed. The management of any secondary infection in this situation should be undertaken with the assistance of a microbiologist. The patient’s tetanus immunization status should be investigated and tetanus toxoid given where appropriate. The risk of contracting rabies in the United Kingdom is extremely low but must be borne in mind when managing such injuries in other countries.
25.3.2 Evaluation of Eyelid Injuries
It is convenient to divide eyelid injuries into the following categories:
Marginal injuries.
Extramarginal injuries.
Avulsion injuries.
Injuries involving tissue loss.
Marginal Injuries
Most full-thickness marginal lid lacerations are easily identified. It is easy, however, to overlook medial canthal injuries, particularly when dried coagulum obscures the area in a child. Relatively minor trauma, even to the lateral aspect of the eyelids, can result in rupture of the attachment of the medial canthal tendon to the tarsus, an area of anatomical weakness, with resulting disruption of the canalicular system. This is particularly true of dog bites, injuries from hooks, and even finger-poke injuries.
Key Point
All marginal trauma to the medial canthal region should be assumed to have damaged the canalicular system unless proved otherwise (see Fig. 25‑3).
Assessing the lacrimal system may be difficult in a child with an injury to the medial canthus, and, in some situations, the patient must be anesthetized for the examination. Failure to identify and repair a canalicular laceration primarily will have long-term consequences for the patient (Fig. 25‑7).

Extramarginal Injuries
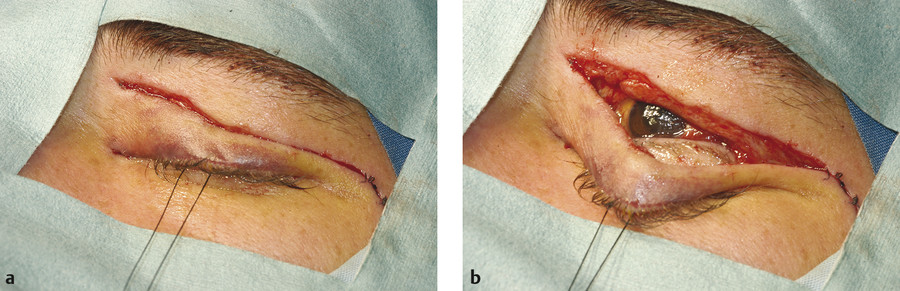
In most instances, extramarginal lid lacerations tend to follow the relaxed skin tension lines (RSTLs) and are oriented parallel to the free margin of the eyelid (Fig. 25‑1). All such lacerations should be considered to be associated with a possible underlying injury to the eye, the orbit, or contiguous structures such as the cranial cavity. Depending on the mechanism of injury and the clinical findings, appropriate imaging studies should be undertaken to evaluate the extent of associated orbital trauma and to rule out the presence of retained foreign bodies. The wound should be gently explored to measure its depth. The presence of fat in the wound indicates that the wound has at least breached the orbital septum (Fig. 25‑8).

In the upper lid it is important not to confuse fat with the lacrimal gland. The fat may be cleaned and gently reposited. It is not necessary to attempt a repair of the orbital septum. If the fat has been exposed for a long period, it may be difficult to reposit it. If it is removed, it should be very carefully cross-clamped with a curved artery clip, first taking care not to apply any traction to the fat. The fat should then be removed with Westcott scissors and the stump cauterized carefully and the artery clip gently released but immediately reclamped in the event of any bleeding. In general, the fat should be left alone to prevent postoperative eyelid asymmetry.
Tissue loss is sometimes seen with extramarginal lacerations, particularly in lacerations from a broken windshield, which produce a characteristic series of partial and sometimes full-thickness linear gouges together with irregular lacerations and abrasions. It may also be seen with some animal bites (Fig. 25‑5).
The results of primary repair are superior to those of secondary repair.
Extramarginal lacerations of the upper eyelid may involve the levator aponeurosis or levator muscle. Any laceration of these structures should be explored and repaired as soon as possible. In an adult it is helpful if the repair can be undertaken using local anesthesia so that the height and contour of the lid can be adjusted appropriately.
Avulsion Injuries
Full-thickness marginal lacerations of the eyelids in the medial canthal area can also be associated with tangential extensions of the lacerations at the level of the eyelid creases and distal borders of the tarsi (Fig. 25‑9). Disruption of the orbicularis muscle allows retraction of the cut edges and gives the appearance of tissue loss. This is, however, very rarely the case.

Injuries Involving Tissue Loss
Although tissue loss in the periocular region is rare, it is important to recognize, because a formal reconstruction may be required. This requires particular oculoplastic expertise (Fig. 25‑5). Attempts to undertake such work by inexperienced hands may seriously compromise the result.
Delay major reconstruction if the necessary expertise is not available.
After the nature and extent of the injuries have been appropriately evaluated, management decisions can be made. The repair of eyelid injuries may be delayed for up to 72 hours if the operating conditions are not optimal. It is preferable, however, to repair such injuries as soon as possible after trauma for the following reasons:
Decontamination of the wounds is far more effective the earlier it is performed.
Posttraumatic tissue edema increases during the first 24 hours after injury.
The surgical repair becomes more difficult to perform after the first 24 hours.
Delay the repair until operating conditions are optimal.
If the ophthalmologist has doubts about the suitability of the facilities in the emergency department or about the patient’s cooperation, the surgical repair should be undertaken in the operating room. If a formal repair of a lacrimal drainage system injury is contemplated, it is preferable to undertake such surgery under general anesthesia. If the surgical repair must be delayed, for example because of potential anesthetic problems, decontamination of the wounds should be carried out and a suitable protective dressing should be applied until surgery can be performed. This is particularly important with respect to bite wounds.
Document all injuries very carefully.
An accurate, detailed, legible history must be recorded and signed. It is particularly important to record any eyewitness statements and to record the names of anyone who administered any first aid. In the case of road traffic accidents, it is important to record who was driving the vehicle. A record of the patient’s vision is mandatory, unless this cannot be measured. A detailed description of the ocular and systemic examination findings with drawings should be recorded.
Photographic documentation of the nature and extent of the injuries is particularly helpful and should always be considered (Fig. 25‑10). Photographic documentation offers significant advantages over drawings:
Photographs provide objective documentation of the patient’s preoperative appearance.
Objective documentation may be useful in supporting claims filed with lawyers, insurance companies, or government agencies.
The photographs can illustrate the ophthalmologist’s testimony should it be required in the future.
Key Point
Accurate and detailed documentation is essential. Many injuries will result in civil or criminal legal proceedings.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


