23 Secondary Anophthalmic Socket Reconstruction
Abstract
“Secondary Anophthalmic Socket Reconstruction” addresses problems that arise some time after an enucleation or evisceration, often involving a volume deficit after loss of the globe; contracture of the socket; orbital implant exposure, extrusion, and malposition; and additional eyelid malpositions. The optimal time to achieve the best functional and cosmetic result for the anophthalmic patient is at the time of enucleation or evisceration, when preoperative planning and a meticulous surgical approach will minimize the risks of complications and reduce the need for secondary surgical reconstruction. Nevertheless, secondary socket surgery represents a significant workload for the oculoplastic surgeon and can be extremely challenging. The patient must be carefully assessed and counseled about the nature of any proposed surgery, its risks, and potential complications. It is important to ensure that the patient has realistic expectations of the surgery. The surgery may have to be carried out in stages. The patient may have to accept a lengthy period without an ocular prosthesis (artificial eye). Such surgery can have profound effects on a patient professionally, socially, and emotionally.
23.1 Introduction
The optimal time to achieve the best functional and cosmetic result for the anophthalmic patient is at the time of enucleation or evisceration. Preoperative planning and a meticulous surgical approach will minimize the risks of complications and reduce the need for secondary surgical reconstruction. Nevertheless, secondary socket surgery represents a significant workload for the oculoplastic surgeon and can be extremely challenging.
Most socket reconstructive surgeries must address the following problems:
A volume deficit after loss of the globe.
Contracture of the socket.
Orbital implant exposure, extrusion, and malposition.
Many patients have additional eyelid malpositions that also require surgery. The patient must be carefully assessed and counseled about the nature of any proposed surgery, its risks, and potential complications. It is important to ensure that the patient has realistic expectations of the surgery. The surgery may have to be carried out in stages. The patient may have to accept a lengthy period without an ocular prosthesis (artificial eye). Such surgery can have profound effects on a patient professionally, socially, and emotionally.
23.2 Patient Evaluation
23.2.1 History
The patient’s current complaints must be documented, including pain, discomfort, discharge, instability of the ocular prosthesis, poor movement of the ocular prosthesis, and poor cosmetic appearance. The following details should be obtained:
The date of the enucleation or evisceration.
The indication for the enucleation or evisceration.
The type and size of any orbital implant used.
The nature of any previous socket or eyelid surgery.
A history of prior radiotherapy treatment.
A history of previous trauma.
23.2.2 Examination
The patient should be examined initially with the ocular prosthesis in place. Any features of postenucleation socket syndrome (PESS) are noted:
Enophthalmos.
An upper eyelid sulcus deformity.
Ptosis or eyelid retraction.
Laxity of the lower eyelid.
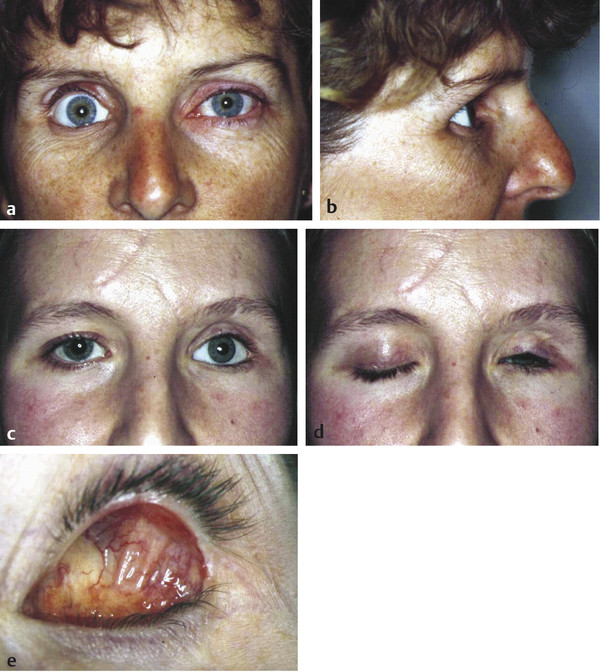
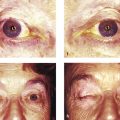
A backward tilt of the ocular prosthesis (Fig. 23‑1a,b).
Any eyelid malpositions or lagophthalmos (Fig. 23‑1c–e).
The degree of movement of the ocular prosthesis is ascertained. The prosthesis is then removed, noting any instability.
The prosthesis is examined for scratches, surface deposits, or other blemishes. Its size and shape are noted.
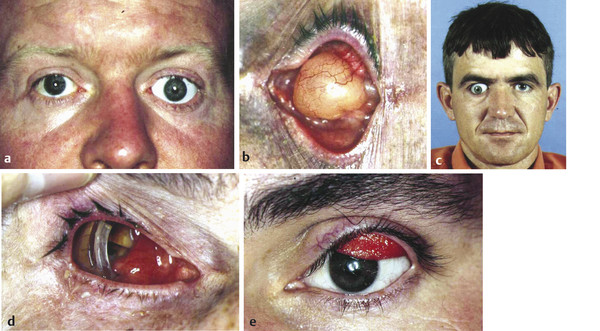
The socket and the conjunctival fornices are examined carefully. Any discharge, bleeding, conjunctival inflammation, implant exposure, granulomas, cysts, sinuses, adhesions, or fornix contracture are noted (Fig. 23‑1c–e; Fig. 23‑2a–d).
The upper eyelid is everted to exclude the presence of papillae (Fig. 23‑2e).
The socket is gently palpated with a gloved finger to confirm the presence or absence of an orbital implant. The patient is asked to look in all directions as the socket is observed to ascertain the positions of the ocular muscles and the degree of movement of the socket. In particular, the position of the inferior rectus muscle is determined. These positions are documented. If the patient has an upper lid ptosis, the patient should be examined thoroughly to determine the underlying cause. A patient who complains of tearing and discharge should be examined to exclude the possibility of an associated obstruction of the lacrimal drainage system.
23.3 Correction of an Orbital Volume Deficiency
Patients who present with a typical PESS may benefit from secondary orbital implant surgery, but the surgical procedure is more difficult and the results are less predictable than primary orbital implantation. Patients undergoing secondary orbital implantation are more likely to require additional surgical procedures. Although the volume deficiency improves after surgery, there is commonly a variable recurrence of the upper lid sulcus defect some months after surgery once postoperative orbital edema has completely resolved.
The type of orbital implant to be used is determined by taking a number of factors into consideration:
The age and general health of the patient.
The condition of the socket.
The size, nature, and complications of any orbital implant already present.
The degree of movement of the extraocular muscles.
The condition of the ocular adnexa.
The cost.
There are five orbital implants of choice for secondary orbital implantation:
Baseball implant.
Hydroxyapatite implant.
Porous polyethylene (Medpor) implant.
Bioceramic implant.
Dermis fat graft implant.
The baseball implant is of use in patients who do not wish to take advantage of the second stage placement of a motility peg. The implant can improve a volume deficiency, but the motility results are unpredictable. If the degree of movement of the implant is good but that of the overlying ocular prosthesis poor, this has to be accepted, because it cannot be improved surgically.
One of the modern porous implants is ideally reserved for a patient who would wish to undergo a second stage placement of a motility peg if the movement of the artificial eye were poor despite acceptable movement of the implant itself. This type of implant is ideal for a patient who has an old extruding or tilted implant. An implant exchange is performed in the absence of any socket infection. The use of this type of implant is ill advised, however, after prior radiotherapy, in the presence of conjunctival inflammation or socket contracture, or for the reconstruction of a badly disorganized socket.
The dermis fat graft is preferred for the reconstruction of a socket that has mild to moderate contracture in addition to a volume deficiency. It is the implant of choice for the reconstruction of badly disorganized sockets and when complications have necessitated the removal of a porous implant or an infected or extruding synthetic implant.
23.3.1 Preoperative Preparation
The patient should be advised about the following:
The advantages, disadvantages, risks, and potential complications of a secondary implant procedure.
The implant options.
The options regarding implant wrapping materials.
Postoperative pain and its management.
The use of a postoperative compressive dressing.
The use of a temporary suture tarsorrhaphy.
The use of a postoperative conformer.
The likelihood of a temporary postoperative ptosis.
The role of the ocularist and the timing of the fitting of the ocular prosthesis.
It is extremely important that the patient remains under the long-term care of an ocularist, who will ensure that the artificial eye is polished at least on an annual basis. Topical lubricants should be prescribed, particularly for a patient who has an incomplete reflex blink. The socket is examined by the ocularist to exclude implantation cysts, papillary conjunctivitis, and implant exposure. Failure to maintain the artificial eye will risk conjunctival inflammation, discharge, conjunctival breakdown, and implant exposure.
The risks associated with such surgery include infection that might necessitate removal of the implant; malposition of the implant that might lead to instability or a poor fit of the ocular prosthesis; exposure that will require further surgery (e.g., a patch graft); socket cyst formation requiring further surgery; and chronic inflammation, pain, or chemosis. Informed consent should be obtained after the patient has had time to consider the options.
The patient should discontinue aspirin and any other antiplatelet drugs if medically permissible at least 2 weeks preoperatively. Likewise, anticoagulants should only be altered or discontinued after discussion with the patient’s hematologist. Any bacterial conjunctivitis should be treated preoperatively and topical steroid drops used every two hours for 2 weeks before surgery to reduce any conjunctival inflammation. In addition, it is preferable for the patient to refrain from wearing an old ocular prosthesis and to wear a well-fitting surgical conformer for at least 2 weeks before surgery.
Key Point
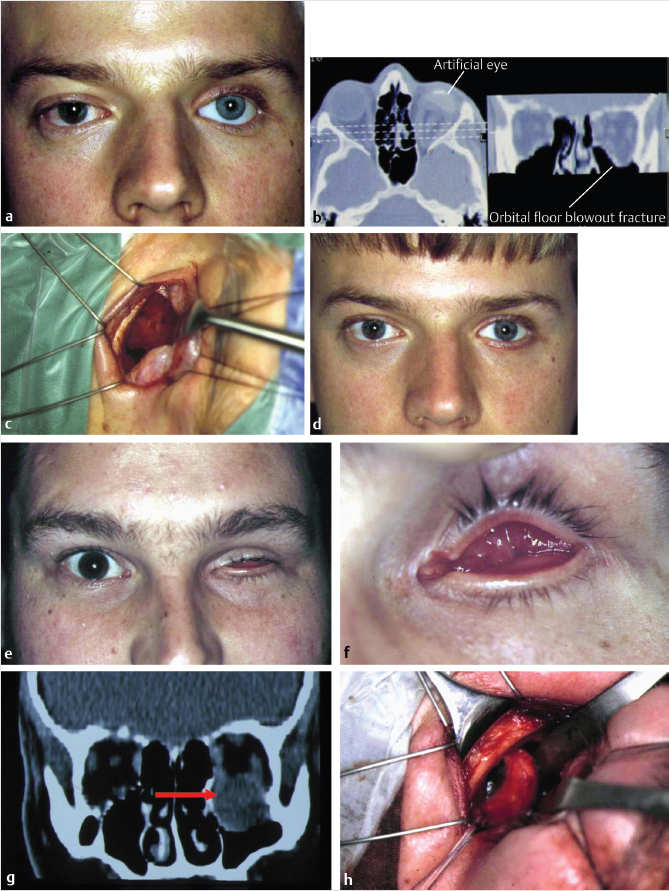
A CT scan of the orbits and paranasal sinuses should be performed if a patient has previously experienced orbital trauma to exclude the possibility of a missed orbital wall blowout fracture (Fig. 23‑3).
If a significant fracture is discovered, this should be repaired before undertaking the secondary orbital implant procedure so that the ideal orbital implant size can be selected and placed in the correct anatomical location in the socket.
23.3.2 Secondary Orbital Implant Procedure
The anesthetist should be warned that the dissection of the socket could provoke the oculocardiac reflex, inducing a severe bradycardia and occasionally asystole. The anesthetist may wish to use intravenous glycopyrrolate or atropine before the dissection. Before the induction of general anesthesia, it is very important that the surgeon examines the patient’s socket while asking the patient to look up and down. The position of the inferior rectus muscle is marked on the conjunctiva using gentian violet. This is to reduce the risk of inadvertently placing the orbital implant beneath the inferior rectus muscle.
Key Point
The surgeon must also ensure that the fellow eye is instilled with a preservative-free lubricant (e.g., Lacri-Lube ointment) and is taped closed and fully protected from inadvertent injury during the course of the surgery.
23.4 Surgical Technique
23.4.1 Spherical Implant
An intravenous injection of a broad-spectrum antibiotic is given by the anesthetist.
The face, eyelids, and conjunctival sac should be thoroughly prepared with an antiseptic agent and a cataract drape applied.
A Clarke’s eyelid speculum is placed to exclude the eyelashes from the surgical field.
Three to five milliliters of 0.5% bupivacaine with 1:200,000 units of adrenaline mixed with 1500 units of hyaluronidase are injected subconjunctivally and deeper into the orbit to prevent the oculocardiac reflex.
A horizontal incision is made through the conjunctiva above the inferior rectus muscle using a no. 15 Bard–Parker blade.
The conjunctiva is dissected into the inferior fornix and then 8 to 10 mm into the superior fornix using blunt-tipped Westcott scissors, taking great care not to damage the underlying levator aponeurosis.
Next 4–0 silk traction sutures are placed through the superior and inferior edges of the conjunctiva using a double pass and fixated to the drapes with curved artery clips.
The central Tenon’s fascia is incised centrally with sharp straight scissors, and then blunt-tipped straight scissors are opened repeatedly to expose the intraconal fat.
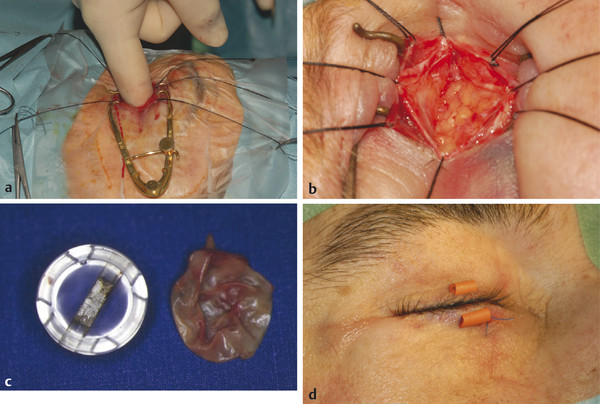
A finger is inserted into the socket to ascertain whether any intraorbital adhesions are present (Fig. 23‑4a). Any adhesions found are dissected bluntly to minimize any trauma to the motor nerves supplying the extraocular muscles.
Four 4–0 silk traction sutures are placed through Tenon’s fascia and fixated to the drapes with artery clips (Fig. 23‑4b).
A double-armed 5–0 Vicryl suture is placed through the approximate anterior positions of all four recti muscles. The muscles themselves are not formally dissected to avoid further trauma.
If an implant is present, this must be very carefully dissected from the surrounding tissues. A Castroviejo/Roper Hall type of implant is relatively easy to remove, and an implant exchange yields very good results, because the recti are easily identified and preserved. The implant capsule should be carefully dissected from the socket (Fig. 23‑4c).
Other types of implant are not as straightforward to remove.
The appropriate size of orbital implant is determined with the use of sizing spheres. If Tenon’s fascia cannot be closed over the surface of the sizing sphere without undue tension, a smaller sphere should be substituted.
The implant of appropriate size is then wrapped in the material that has been selected by the patient during the preoperative consultation, whether donor sclera, Vicryl mesh, or autogenous fascia lata or AlloDerm.
The implant is then inserted into the intraconal fat space using a Carter sphere injector.
The Vicryl sutures are attached to the implant as far anteriorly as possible, and additional interrupted 5–0 Vicryl sutures are placed as required to ensure that the posterior Tenon’s fascia is completely closed over the implant.
A patch graft of donor sclera or autogenous fascia is then placed over the suture line to reduce any risk of implant exposure.
Anterior Tenon’s fascia is then closed with interrupted 7–0 Vicryl sutures, and finally the conjunctiva is closed, likewise taking great care to ensure that the inferior fornix is not inadvertently shallowed.
A sterile surgical conformer of appropriate size and shape is inserted into the conjunctival sac, ensuring that the eyelids will close passively over the conformer without creating tension on the conjunctival suture line.
A temporary suture tarsorrhaphy should be undertaken using a central 4–0 nylon suture passed through tarsorrhaphy tubing (Fig. 23‑4d).
A retrobulbar injection of 5 mL of 0.5% bupivacaine with 1:200,000 units of adrenaline is given to aid postoperative analgesia.
Injections of an anti-inflammatory agent and an opiate analgesic are given by the anesthetist. An intravenous injection of steroid also acts as an antiemetic as well as helps to reduce postoperative swelling.
Topical antibiotic ointment is instilled into the conjunctival sac on either side of the tarsorrhaphy.
Jelonet is placed over the eyelids along with two eye pads and Micropore tape, and a compressive head bandage is applied before the patient’s anesthesia is reversed.
Postoperative Care
The patient will usually experience postoperative nausea and pain and is not usually discharged until the second postoperative day. It is extremely important not to underestimate the degree of pain that can be associated with an enucleation or evisceration with placement of an orbital implant, and adequate analgesia must be provided as soon as the effects of local anesthesia begin to wear off.
The patient is discharged on a week’s course of a broad-spectrum oral antibiotic, a 2-week course of an oral anti-inflammatory agent, and analgesics (usually a combination of paracetamol and codeine). The patient is instructed to remove the bandage and the dressing 3 days after surgery, and to clean the eyelids and tarsorrhaphy tubing with cotton wool and sterile saline or cooled boiled water. Topical antibiotic ointment is then smeared across the eyelid margins for 2 weeks. The temporary suture tarsorrhaphy is removed in the office 2 to 3 weeks postoperatively and the topical antibiotic ointment is changed to topical antibiotic drops. These are continued for a further 2 weeks.
Key Point
It is extremely important not to underestimate the degree of pain that can be associated with an enucleation or evisceration with placement of an orbital implant, and adequate analgesia must be provided as soon as the effects of local anesthesia begin to wear off.
The patient’s conformer is then checked, cleaned, and replaced or changed for a different size and shape if required. The patient should not be fitted with an ocular prosthesis until a minimum of 8 weeks have elapsed to allow sufficient wound healing and complete resolution of postoperative edema. If the ocular prosthesis is fitted too soon after surgery, the risk of implant exposure is increased. In addition, the ocular prosthesis will not fit the socket properly once complete resolution of postoperative orbital edema has occurred, increasing the likelihood of postoperative socket inflammation and discharge.
The patient should remain under the care of the ocularist, who will ensure that the ocular prosthesis is checked and polished at least on an annual basis. If the patient has an incomplete blink or lagophthalmos, the ocular prosthesis should be polished more frequently. Topical lubricants should be prescribed, particularly for a patient who has an incomplete blink. The socket should be examined to exclude implantation cysts, papillary conjunctivitis, and impending or actual implant exposure. Failure to maintain the artificial eye will risk conjunctival inflammation, discharge, conjunctival breakdown, and implant exposure.
Key Point
The regular long-term postoperative care of the ocular prosthesis by an ocularist is crucial to the success of orbital implant surgery.
The degree of movement of the implant may be poor initially as a consequence of neuropraxia or direct trauma to the extraocular muscles. This commonly improves over the course of the next few months.
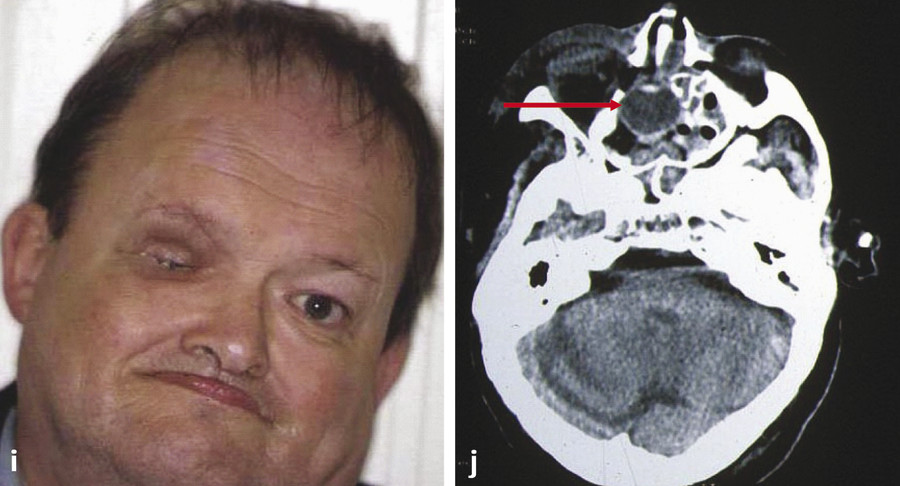
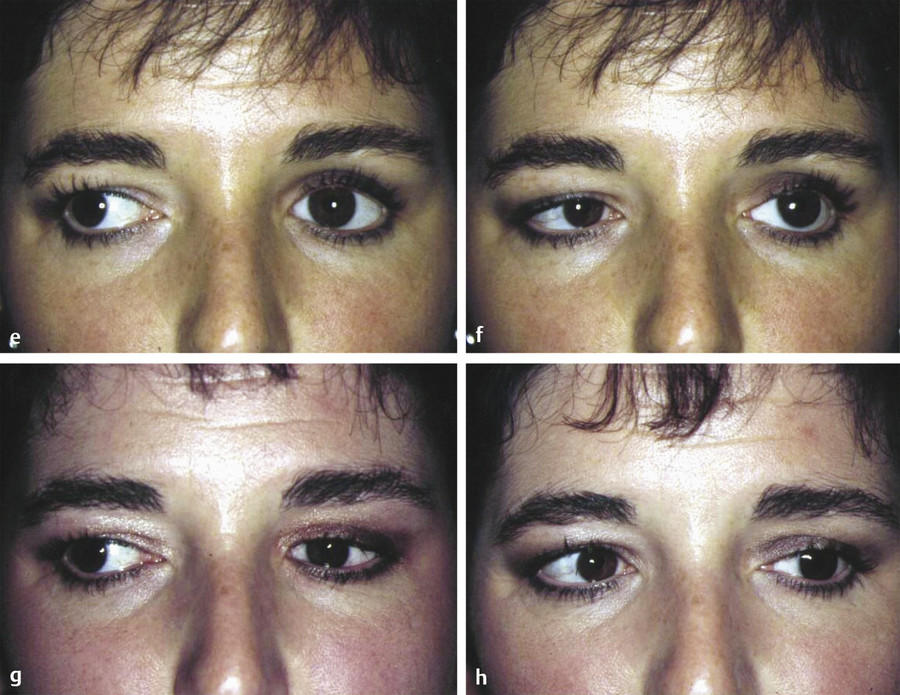
The improvement in the features of a PESS after placement of a secondary orbital implant is demonstrated in Fig. 23‑5a–d. The improvement gained by the exchange of a Castroviejo for a hydroxyapatite orbital implant is demonstrated in Fig. 23‑5e–h.

23.4.2 Dermis Fat Graft
Surgical Procedure
A 25-mm circle is outlined on the inferior quadrant of the abdomen or on the upper outer quadrant of the buttock. The circle is extended to form an ellipse to facilitate wound closure.
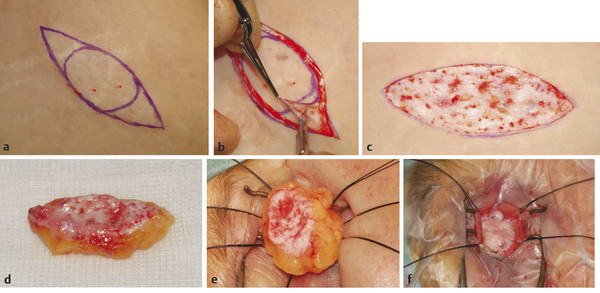
Three milliliters of 0.5% bupivacaine with 1:200,000 units of adrenaline are injected subconjunctivally in the socket, and a further 10 mL are injected intradermally in the anterior abdominal wall at the proposed site of the graft excision to create a “peau d’orange” appearance (Fig. 23‑6a).
Next, a skin incision is made along the marks and the epidermis carefully shaved off the proposed graft in a single sheet using a no. 15 Bard–Parker blade (Fig. 23‑6b). The pale dermis should now show multiple fine bleeding points, and ideally very little of any fat should be visible (Fig. 23‑6c).
An incision is made through one edge of the dermis, and the dermis fat graft is removed using Stevens scissors (Fig. 23‑6d).
The wound is closed using interrupted subcutaneous 4–0 Vicryl sutures and interrupted 4–0 nylon sutures for the skin.
The graft is subsequently cut to the desired shape required for a socket implant (Fig. 23‑6e,f).
The socket is prepared and dissected as for a secondary spherical implant.
The dermis fat graft is then inserted into the socket and the Vicryl sutures are attached to the anterior surface of the graft (see Fig. 23‑18).
If there is a conjunctival lining deficit the sutures are positioned closer to the edge of the graft to leave a central bare area of graft exposed. This epithelializes gradually. As the sutures are tied, the fat is reduced into the intraconal fat space. The conjunctiva is sutured to the front surface of the graft with interrupted 7–0 Vicryl sutures leaving an area of the graft bare in the presence of socket contracture. In the absence of a lining deficit the conjunctiva is closed over the dermis fat graft.
A surgical conformer of appropriate size and shape is placed, ensuring that the eyelids close passively.
The rest of the procedure is completed as for a secondary spherical orbital implant procedure.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


