22 Office Rhinoplasty Techniques
Key Concepts
Office-based rhinoplasty techniques can be used to address postoperative minor rhinoplasty revision issues.
There are many less extensive nasal procedures that can be performed with simple local anesthesia in an office setting.
Soft tissue fillers have provided another means for correcting subtle contour irregularities.
Introduction
The majority of rhinoplasty procedures will continue to be done in operating rooms, utilizing either general or monitored anesthesia techniques. Patients demand this for comfort and reduction of anxiety. Surgeons prefer anesthesia for rhinoplasty because it often creates a more comfortable surgical environment. Patient safety with airway safeguards is also emphasized in accredited surgical centers. This description applies to most primary and many revision rhinoplasty operations. On the other hand, there are many less extensive nasal procedures that can be performed with simple local anesthesia in an office setting. These techniques typically address postoperative rhinoplasty patients who need a minor revision or management of common postrhinoplasty healing patterns. If it can be done with local anesthesia in an office or exam room environment, it fits the scope of this chapter. All procedures described in this chapter are designed so that the patient can be discharged immediately to home, without complex postoperative care.
Technical Aspects of Procedures
Early Postoperative Procedures
The healing process in rhinoplasty is slow and frequently tests the patience of both surgeon and patient. Soft tissue edema, in addition to gradual scar contraction around the skeletal framework, may take years to finalize. Certain postoperative therapies and maneuvers can impact healing as this process unfolds.
One area that is frequently a problem is the supratip. In patients with marginal tip projection and thicker skin, this may show up early in the postoperative period. The mainstay of early treatment for this problem is prolonged taping and subcutaneous steroid injection. In our practice, it is not unusual to initiate steroid injections 1 week after surgery if the surgeon feels that it will help reduce supratip edema and prevent a deformity down the road. The initial treatment involves injection of 0.1 mL triamcinolone 10 mg/mL into the subcutaneous space just above the tip. It is important to avoid an intradermal injection because this may cause dermal atrophy and a significant contour defect. Over time, these defects may improve, but prevention is the best policy ( Fig. 22.1 ).1
Taping of the nose after surgery is one of the mainstays of postoperative treatment. The purposes of taping are generally acknowledged to be stabilization, elimination of a potential space, and containment of edema in key areas. The supratip is probably the area where taping is most effective. After the initial dressing is removed at 1 week after surgery, retaping the nose is an option. Combined with steroid injection, taping for an additional 1 to 2 weeks can be quite effective in the treatment of early supratip edema.

When rhinoplasty surgery involves osteotomies, malposition may occur early in the postoperative period. At the first visit after surgery, the surgeon can use digital pressure to realign the bones, usually after topical and regional local anesthetic is employed. Even with the local anesthetic, this can be uncomfortable for the patient. If the bones are too medial in position, intranasal pressure with a blunt instrument can be utilized to lateralize the bones, with reapplication of tape and splint for 1 more week.
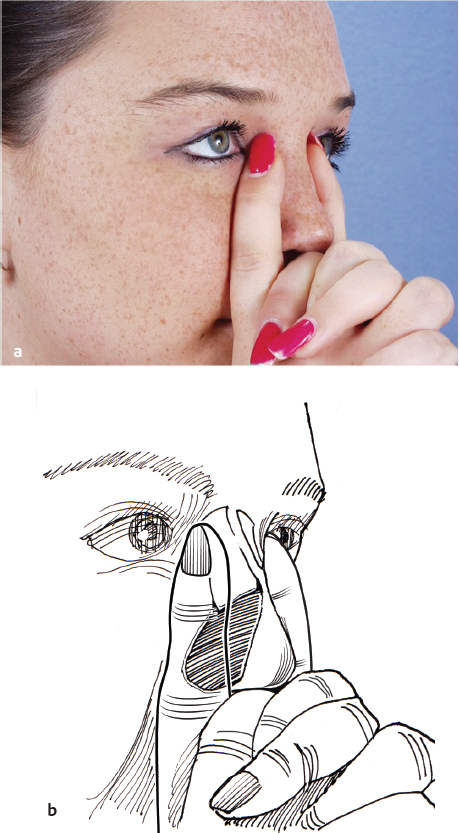
Having the patient apply digital pressure on a regular basis can also treat subtle deviations of the bony structures. We routinely ask all rhinoplasty patients to apply bilateral pressure every 2 hours during the day for a period of 4 weeks. This must be demonstrated at the first postoperative visit to ensure the pressure is applied correctly ( Fig. 22.2a,b ).
Late Postoperative Procedures (> 6 Months)
Telangiectasias
Increased vascularization of the nasal dorsum soft tissue can occur after rhinoplasty, regardless of the surgical approach used ( Fig. 22.3 ). This redness can be exacerbated by certain skin care products, sun exposure, hot flashes, and hot beverages or alcohol. Patients who find these telangiectasias troublesome often use cosmetics to camouflage the redness. If isolated telangiectasias occur, simple cauterization of the vessel(s) can be performed. The Hyfrecator unipolar cautery can be fitted with a 30-gauge metal hub needle by adding a small adapter to the handpiece. This allows direct cauterization of the targeted vessels without the need for topical or local anesthesia and does not injure the surrounding tissue.
Laser treatment is required when the telangiectasias are more diffuse. The flashlamp pulsed dye laser and the V Beam lasers (Syneron, Inc., Irvine, CA) are ideal for this situation. In addition, an yttrium-aluminum-garnet (YAG) laser can be used to treat this condition with excellent results, although more than one treatment may be necessary.
Cartilage Irregularities
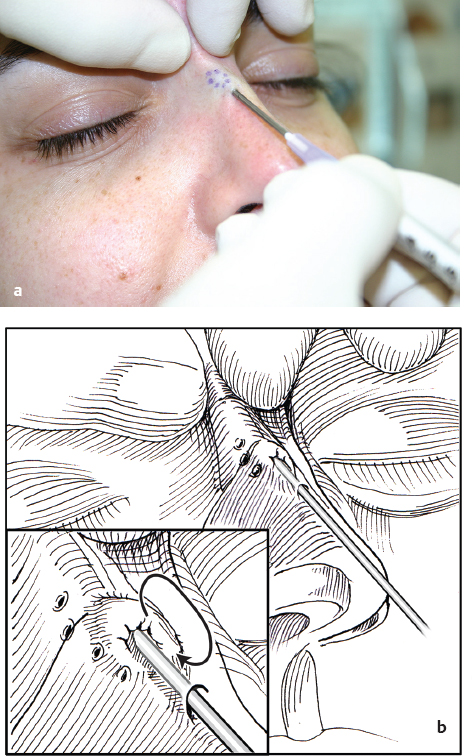
As the soft tissue envelope thins over time, cartilage irregularities can become evident, especially in thin-skinned individuals. Both the dorsum and the nasal tip can have cartilaginous abnormalities that become noticeable in the late postoperative period. Most cartilaginous irregularities can be treated in the office in the minor procedure room under local anesthesia. Very small nodular irregularities can be treated using the needle shaving technique Video 22.1. The cartilaginous lump is marked with a surgical marker, and local anesthesia is infiltrated. A 20-gauge needle is inserted into the skin, and the bevel of the needle is used to shave off the prominent cartilage ( Fig. 22.4a,b ).

Larger cartilaginous irregularities require an open procedure, usually performed in the minor procedure room. The irregularity is marked prior to injection. After local anesthesia is infiltrated, an intercartilagenous incision is performed, unilateral or bilateral, depending on the exposure needed. The nasal dorsum tissue is undermined, and the cartilaginous irregularity is excised and the fragment removed. The incisions are closed with 4–0 chromic suture. This procedure is tolerated well with either local anesthesia or with the addition of oral lorazepam preoperatively.
The nasal tip skin is the last area of the nose to regain its definition as the edema subsides. Occasionally, tip irregularities can become manifest late in the healing process. A nasal tip revision can also be performed in the local room with or without preoperative premedication with lorazepam. Surgical access can range from reopening the nose through the transcolumellar incision to delivering the tip for better visualization.
Camouflage of cartilaginous irregularities of the nasal tip can be achieved with the use of fascia or allograft. Fascia can be harvested from the temporalis muscle or from conchal perichondrium. Several types of allograft are also available for use. The fascia or allograft can be placed into a pocket dissected over the nasal tip cartilage, but care must be taken to ensure smooth, unfolded placement. More accurate placement can be achieved if the cartilages are better exposed by the open or delivery techniques, whereby the graft can be sewn into place over the nasal tip cartilages ( Fig. 22.5a–d ).2
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


