21 Omental Flap Reconstruction
Oncoplastic surgery encompasses unique approaches and focuses on tumor resection and breast aesthetics through partial breast reconstruction techniques that minimize potential breast deformity, as described by Audretsch. 1 Volume replacement technique is often needed for smaller breasts or for patients with a small breast-to-tumor ratio.
They often consist of partial breast reconstruction with pedicled distant flap. The latissimus dorsi (LD) flap has played a main role in volume replacement, but has the disadvantages of donor-site morbidity and deformity, such as seroma formation and an obvious scar on the back. 2 An ideal flap for volume replacement should have (1) less donor-site morbidity and deformity, (2) strength against radiotherapy, (3) applicability to any quadrants of the breast, (4) preservation of total reconstructive options, (5) at least equal or better cosmetic outcome than that of total reconstruction, and (6) more simplicity than that of total reconstruction. No single flap can meet all the conditions described above. Surgeons must select the appropriate technique for the appropriate patients.
For example, lateral chest wall perforator flaps, including the thoracodorsal artery perforator (TDAP) flap and the lateral intercostal artery perforator (LICAP) flap have been well developed to minimize the donor-site morbidity. 3 However, it is generally difficult to utilize these perforator flaps in partial breast reconstruction for lower medial located tumors because adequate mobilization and a longer pedicle are needed to reach and replace the distant defect of the breast tissue. 4
Defects in the lower medial quadrant can be addressed using the abdominal adipofascial flap 5 , 6 and the anterior intercostal artery perforator (AICAP) flap. 7 However, it is still difficult to utilize these flaps for the upper medial quadrant, which constitutes a major part of a no-man’s land of the breast.
The omental flap is unique but not a newly developed flap. Historically, many applications for the omentum have been reported because of its protective and beneficial roles against infection and regenerative properties of ischemia. 8 Nevertheless, the omental flap could not obtain widespread popularity because of its severe laparotomy-associated donor-site morbidities and deformity such as ventral hernia and bowel obstruction. 9 However, rapid advances in endoscopic surgery have allowed laparoscopic harvesting of the omental flap with minimal donor-site deformity and morbidity, which has made the omental flap revive and more attractive. 10
The omental flap can be harvested laparoscopically with minimal donor-site deformity and morbidity.
It was not until 1993 that Salz et al 11 published a case of a laparoscopically harvested omental free flap. Since then, there have been several case series in which the omental flap was used for breast and/or chest wall reconstruction. 12 , 13 Taking both the advantages and the disadvantages of this flap into account, the best indication of the omental flap is immediate partial breast reconstruction after breast-conserving surgery (BCS). 14 , 15
Patient Selection
The omental flap is usually used when a 20% or wider region of the breast tissue is resected or the cosmetic result is poor because of the location of the tumor in the medial quadrants. When the patient’s breast size is small, even a 10% resection of the breast tissue in the lower medial quadrant might cause cosmetic disaster.
The biggest advantage of this flap is minimal donor-site deformity. To obtain this advantage, patients must be carefully selected based on a combination of factors.
Factors Related to the Tumor
When a large amount of skin over the tumor needs to be resected, this procedure is not appropriate because the omental flap cannot replace the skin.
Factors Related to the Size of the Defect
One of the disadvantages of this procedure is an inability for preoperative estimation of the volume of the omentum. Some patients have a large omentum which weighs more than 500 g and can easily accomplish total reconstruction, but some patients have only 100 g of the omentum. Patients who are large or obese tend to have a larger omentum, but estimation only by body size does not always fit. Our limited data, derived from only Japanese patients, suggest that it should be cautious when the volume of the defect exceeds 100 g for the very thin patients, and for the large patient, care must be taken when the volume of the defect exceeds 200 g.
It is difficult to estimate the accurate volume of the omental flap preoperatively. Care has to be taken when more than a quadrant of resection is necessary.
Factors Related to the Location of the Defect
The omental flap can reach any quadrants, however, the lower medial quadrant is the most suitable defect because of its anatomic advantage. The upper medial and the lower lateral quadrant are also comfortable locations. For the upper lateral quadrant, a long subglandular tunnel must be created under the breast tissue for the omental flap to pass and reach the defect, just like for the LD flap to replace the lower medial quadrant. So it is usually more complicated to apply the omental flap for the upper lateral quadrant than for the other quadrants.
The omental flap is most suitable for the medial quadrants, which are difficult to reconstruct for the other pedicled flaps.
Factors Related to the Patient
Patients who have either a history of intraabdominal malignancy or upper abdominal laparotomy are excluded. However, a history of laparoscopic surgery (such as laparoscopic cholecystectomy) and a history of lower abdominal surgery (such as cesarean section) do not necessarily have to be excluded, because intraabdominal adhesions tend to be mild in such cases. Patients who wish to be pregnant in the future are also indicated.
Although obese patients are not contraindicated, our current practice basically excludes patients with a body mass index (BMI) of 35 or more, because it is difficult to extract a huge amount of the pedicled omental flap without making a mini-laparotomy incision on the upper abdomen, which prevents minimization of the donor-site scar.
The omental flap is most appropriate for small- or medium-sized breasts.
Preoperative Planning
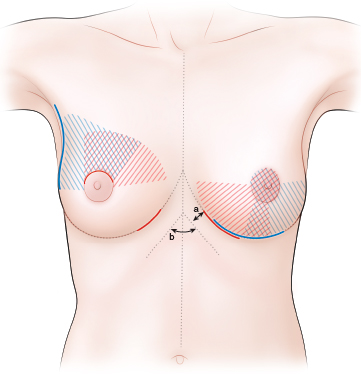
The IMFs and midline on the sternum are marked in the standing position. The choice of incision on the breast is influenced mainly by the location of the tumor. An inframammary incision for the lower quadrants is the preferable choice for the omental flap. For the upper quadrants, many types of incisions, such as circumareolar and lateral S-shaped, can be adapted, depending on the surgeon’s preference or oncologic consideration. A separate small incision on the medial IMF to extract the omental flap as well as a skin incision for partial mastectomy are also necessary.
A length between the IMF and the costal margin is also checked in the supine position to make a plan to create a subcutaneous tunnel (arrow a). The tumor and resection margins are outlined on the skin of the breast.
Surgical Technique
Surgery is performed with the patient in the supine position with both arms abducted at 90 degrees. A general anesthetic is administered.
Partial Mastectomy
Lower Quadrants
Dye mixed with lidocaine is injected around the planned resection margins to make appropriate resection. The injection markings should reach the pectoralis fascia. An incision is made along the IMF.
An inframammary incision is always preferable for the partial mastectomy in the lower quadrants because it is invisible and gives easy access to the abdominal cavity.
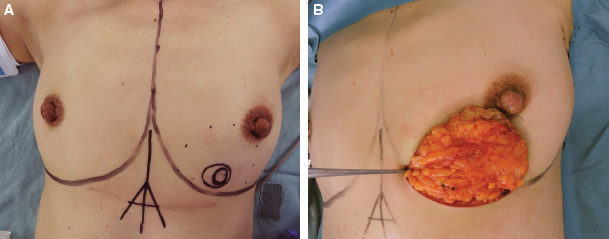
For the tumor in the lower medial quadrant, a 6 to 7 cm skin incision is made on the medial IMF (red line on the left IMF in Figs. 21-1 and 21-2, B). For the tumor in the lower outer quadrant, a medial end of the incision is placed at the closest point to the lower pole of the xiphoid process and an approximately 10 cm long incision is made on the IMF laterally (blue line on the left IMF in Fig. 21-1). The dissection is extended above or behind pectoralis fascia depending on oncologic consideration. The previously dye-marked outline of the resection margins on the pectoralis fascia help to define the area of this dissection. It is better to avoid unnecessary dissection from the pectoralis fascia for subsequent reconstruction. Then the subcutaneous dissection is performed, also depending on the marked outline. Thus the tumor-bearing quadrant has been separated completely from the deep and superficial tissue, and a partial mastectomy is completed by grasping the dissected breast tissue.
Upper Quadrants
A circumareolar incision is the preferable choice for partial mastectomy (red line on the right breast in Fig. 21-1). A lateral S-shaped incision is also applied for the tumor in the upper outer quadrant (blue line on the right breast in Fig. 21-1).
A separate 3 to 4 cm long incision on the medial IMF as well as an incision on the breast is also necessary for the tumor located in the upper quadrants to extract the omental flap (red line on the right IMF in Fig. 21-1).
Laparoscopic Harvesting of the Omental Flap
The principles of laparoscopic surgery are followed. 13 Surgery continues with the patient in the same position. Three ports are usually used.
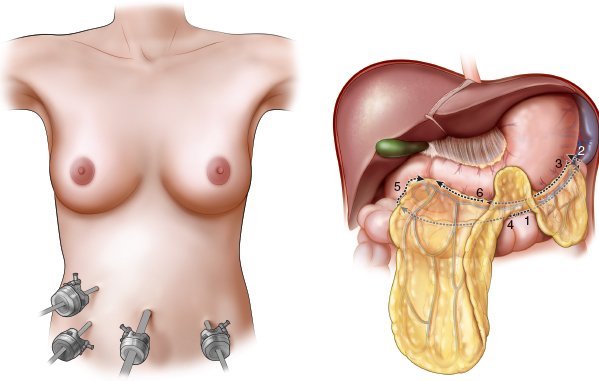
The omentum is first dissected from the left side of the transverse colon, followed by ligation of the left gastroepiploic vessels. The second step is to separate the omentum from the stomach to reach the right side from the omentum.
After complete dissection from the transverse colon, dissection from the stomach is advanced across the pyloric ring. Very careful dissection is required at this point, because the gastroepiploic artery and vein (GEAV) run close to the wall of the stomach and the proximal duodenum, and the branches tend to bleed easily.
It is better to resect as much fatty tissue around the root of the GEA V as possible for the long, thin pedicle of the Hap to avoid a ventral hernia.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


