15 Reduction Techniques to Optimize Results
Poor outcomes after breast-conserving therapy (BCT) are likely to be underestimated in the literature, because many patients with such outcomes are reluctant to seek additional surgical treatment. Breast preservation may provide sufficient psychological satisfaction for some women; however, others may fear additional operations or may not be aware of the reconstructive options available to them. 1 Many patients choose to undergo BCT to limit the extent of surgery. Therefore these women are not eager to undergo a major secondary reconstructive procedure, which may be necessary after radiotherapy.
Many patients wish to preserve their breasts, regardless of the anticipated cosmetic outcome. This has led to the more aggressive use of partial mastectomies and to more extensive local resections being classified as partial mastectomies. 1 As partial mastectomies become more extensive, the risk of suboptimal cosmetic results most likely will increase. 2 The importance of incorporating immediate reparative techniques in the multidisciplinary care of these patients has never been so critical.
The Decision-Making Process
In addition to an improved cosmetic outcome, the immediate repair of partial mastectomy defects using the breast-reduction technique offers a number of potential advantages. It can facilitate the resection of wider margins around the tumor, which in turn has the potential to lower the rates of local recurrence of breast cancer. 3 The immediate repair of partial mastectomy defects may also increase the eligibility of large-breasted patients for BCT. Some radiation oncologists are reluctant to treat large-breasted patients because of the potential for poor aesthetic outcomes. Because of the increased fat content, radiation delivered to a large breast can lead to increased fibrosis; it can also be difficult to duplicate the setup from one daily treatment to the next. 4 A reduced breast size allows a more uniform radiation dose to be delivered at lower levels, thereby reducing unacceptable late radiation reactions. 5 , 6 The immediate repair of a partial mastectomy defect using breast-reduction techniques represents an alternative for those patients who would otherwise not be considered candidates for BCT.
Immediate repair with the breast-reduction technique does not pose a problem with postoperative cancer surveillance, 5 and it may provide some medical benefits.
A contralateral breast reduction is often required. Although this increases the potential for complications, it allows tissue from the contralateral breast to be sampled. Occult carcinomas have been found in approximately 4.5% of contralateral breast reduction specimens in patients undergoing a symmetry procedure for breast reconstruction. 4 Although the detection of occult carcinoma is not itself a reason to perform a contralateral breast reduction, it may provide a benefit for high-risk patients. Breast-reduction surgery has also been shown to significantly reduce the risk of breast cancer, especially in women older than 40 years of age. 7
This chapter introduces a management algorithm to guide the clinician in determining which patients are good candidates for having the breast-reduction technique to repair a partial mastectomy defect. It focuses on patient selection and presents new zone designations of the breast, with corresponding designs for dermoglandular pedicles based on the tumor location.
*Complications include nipple necrosis, donor or recipient site seroma, wound dehiscence, infection, hematoma, fat necrosis, and mastectomy skin-flap necrosis.
The results of our studies 8 , 9 indicate that, in eligible patients, breast-reduction techniques result in the fewest complications.
*As opposed to the calculation of complication rates, which were based on each reconstructed breast, a cosmetic outcome score was determined for each patient. Cosmetic outcomes were evaluated for 10 patients who underwent immediate reconstruction and 9 patients who underwent delayed reconstruction.
†Mean intervals: from reconstruction to photograph, 10 months; from radiotherapy to photograph, 2 years 3 months. Mean defect size: 21%.
‡Mean intervals: from reconstruction to photograph, 12 months; from radiotherapy to photograph, 8 months. Mean defect size: 23%.
§Mean intervals: from reconstruction to photograph, 8 months; from radiotherapy to photograph, 4 years. Mean defect size: 19%.
BR, Breast reduction; FLAP, reconstruction with a latissimus dorsi myocutaneous or thoracoepigastric flap; LTR, local tissue rearrangement.
Breast-reduction techniques also yield the best cosmetic outcomes, because they use the remaining breast tissue to maintain the color and texture of the breast.
Management Algorithm
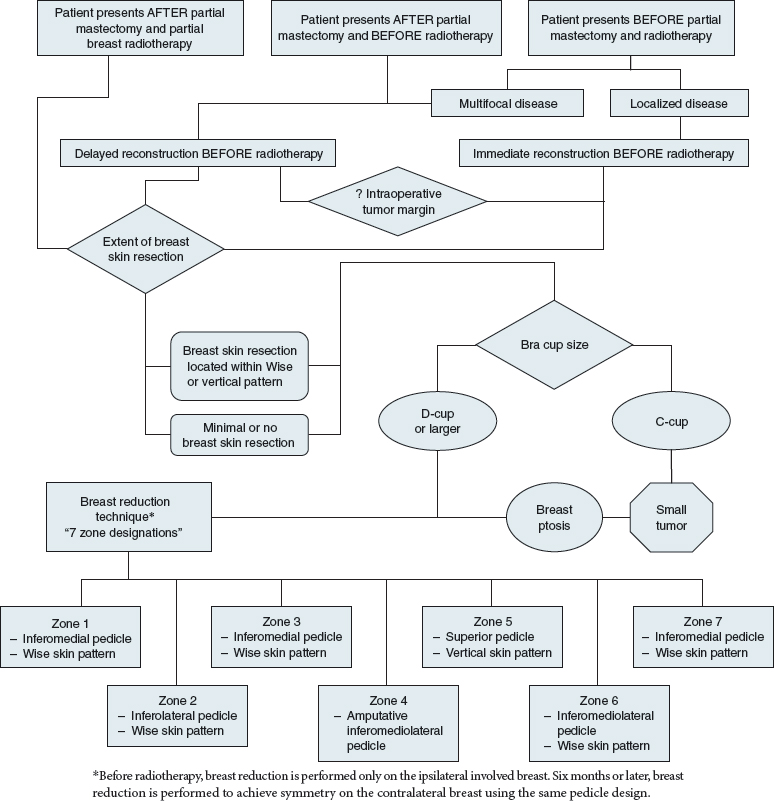
Although no exact measures are available to determine which patients will benefit from repairing a partial mastectomy defect using the breast-reduction technique, the algorithm presented should prove useful in determining eligibility. This technique usually is limited to patients with large-sized breasts (D-cup bra size or larger). However, some patients with moderate-sized breasts (C-cup bra size), small tumors, and nipple ptosis may also be candidates for the breast-reduction technique. Ultimately it is up to the multidisciplinary breast team and the patient to determine the best approach.
Three groups of patients are presented in the algorithm. The first group includes patients who present after undergoing a partial mastectomy and partial breast radiotherapy; this group consists of an increasing number of women who, in the near future, may become the largest presenting population for the repair of partial mastectomy defects. Because the radiotherapy is delivered only to the tumor site, the remainder of the breast parenchyma can be rearranged in these patients without significant concerns of poor wound healing. Another advantage for patients in this group is that a negative margin has already been obtained and the tumor cavity does not need to be elucidated (with placement of surgical clips) for the radiation oncologist. The disadvantage is that an incision on the breast has already been made, which may interfere with the design of the skin resection pattern. The decision-making with these patients is based on the extent and location of the breast skin resection and the breast size. Patients with D-cup breasts and C-cup breasts with small tumors and breast ptosis are excellent candidates for the breast-reduction technique. The second group of patients, those who present after a partial mastectomy and before radiotherapy, also has an advantage and disadvantage in terms of the reconstruction. The advantage is that negative tumor margins have usually already been obtained in these patients. However, the disadvantage is that the specific location and extent of the tumor resection often are not known. This is especially important when determining whether an adequate blood supply from the underlying breast parenchyma remains for the NAC.
In patients who have undergone a central resection or, by examination, have evidence of a subareolar resection, the blood supply to the NAC should be explored before the surgeon commits to performing a breast-reduction technique.
Otherwise, when choosing the best technique for repairing a partial breast defect in these patients, consideration must be given to the location and extent of the tumor resection and to the breast size.
The third group of patients present before undergoing a partial mastectomy and radiotherapy. This scenario is ideal, because it allows the multidisciplinary approach of caring for the patient with breast cancer to be applied. However, several important considerations must be given to this patient population. Most patients who undergo a partial mastectomy have localized disease. However, if a woman presents with multiple foci of disease, she is probably better served with delayed repair; there is an increased risk of both a positive tumor margin and a severe breast deformity, and she would more likely benefit from a total mastectomy with immediate or delayed immediate breast reconstruction.
The most important consideration for these patients is the status of the tumor margin. The decision to either proceed with an immediate repair or to wait 1 or 2 weeks until a negative margin has been confirmed rests with the breast surgeon, the pathologist, and the reconstructive breast surgeon in consultation.
Although it may seem intuitive to delay the repair until after a negative tumor margin is confirmed, many patients are at a low risk and would require an additional surgery to perform the repair before radiotherapy. After these issues have been addressed, the location and extent of the skin resection and the breast/tumor ratio must be considered.
Timing of the Reconstruction
Waiting to repair a large partial mastectomy deformity until after whole breast radiotherapy usually necessitates a complex transfer of a large volume of autologous tissue, and many patients who undergo BCT are not willing to undergo this procedure. The difficulties associated with a secondary repair in an irradiated surgical field often limit the use of adjacent irradiated breast tissue, because complication rates are high and breast implants are not a preferred option. However, with the increasing use of partial breast irradiation instead of whole breast irradiation, using the remaining breast tissue (breast-reduction technique) may become a viable option for these patients. Although we usually prefer immediate repair, if an unexpected deformity results after a partial mastectomy or if the tumor margin status is unclear at the time of the partial mastectomy, reconstruction still can be performed before radiotherapy once the final margin status has been confirmed.
Tumor Margin Status
Attention must be given to the tumor margin status before rearranging the breast parenchyma. If there is ever any concern—either preoperatively or intraoperatively—about the ability to determine the adequacy of the tumor margins, the partial mastectomy wound is closed primarily, without any tissue rearrangement. After negative margins are confirmed on the permanent sections, the repair is performed within several weeks of the partial mastectomy; usually there is no delay in starting radiotherapy.
*Based on the initial 84 patients, before excluding patients who did not receive radiotherapy, because it did not affect the rate of positive postoperative tumor margins.
†Based on the 69 patients who received radiotherapy. Positive postoperative tumor margins are only pertinent to immediate reconstruction after partial mastectomy.
‡Borderline statistical significance (p = 0.06).
§Positive postoperative tumor margins are only pertinent to immediate reconstruction after partial mastectomy. BR, Breast reduction; FLAP, reconstruction with a latissimus dorsi myocutaneous or thoracoepigastric flap; LTR, local tissue rearrangement.
BR, Breast reduction; FLAP, reconstruction with a latissimus dorsi myocutaneous or thoracoepigastric flap; LTR, local tissue rearrangement.
In our series, 8 only 5% of patients had a positive tumor margin after undergoing immediate repair after partial mastectomy. This relatively low rate of positive tumor margins reflects the large defect sizes that are usually present in patients who undergo a partial mastectomy and require repair. This rate is lower than rates for positive margins in patients who do not undergo repair, 10 because the defect sizes that are reported in patients who do not undergo repair are usually smaller.
The low rate of positive tumor margins alleviates concerns regarding the potentially awkward situation of trying to locate the position of a positive tumor margin after an immediate repair with the breast-reduction technique. In addition, our experience indicates that the majority of the patients who are scheduled for repair because of larger anticipated defects usually proceed to a completion mastectomy with immediate breast reconstruction and not additional reexcision. The relatively low incidence (5%) of the local recurrence of breast cancer 8 is further evidence of its safety and should support the role of immediate repair of partial mastectomy defects using the breast-reduction technique as a definitive method of breast reconstruction.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


