17 Central Defect Reconstruction
Oncoplastic approaches and principles are no better demonstrated than in the breast-conserving approaches to central breast tumors that require the removal of the nipple-areolar complex. These procedures represent less than 5% of patients with breast cancer; however, from a cosmetic outcome perspective, they have traditionally been regarded as a difficult group to treat.
Patient Selection and Planning
The ideal oncoplastic procedure potentially improves the oncologic and cosmetic outcomes for a patient. Such techniques extend the role of breast conservation by allowing standard or even extended oncologic excisions in patients at high risk of a breast deformity. The techniques also reduce the need for reexcision especially in DCIS and with larger volume excisions. Patients benefiting from oncoplastic techniques include those who require an excision of a significant percentage of their breast 1 or who have tumors in sensitive areas such as the central part of the breast. The cosmetic outcomes for central tumors have been so poor traditionally that mastectomy was often regarded as the first line treatment. BCTs are now increasingly applied to central tumors when it is oncologically feasible to do so. 2 In some cases the balance between mastectomy and reconstruction and oncoplastic breast-conserving surgery may be a fine one, particularly in smaller breasts or large-percentage excisions. However, even with these patient groups, oncoplastic techniques can be applied with predictable outcomes, and women can be given a choice. 3 , 4
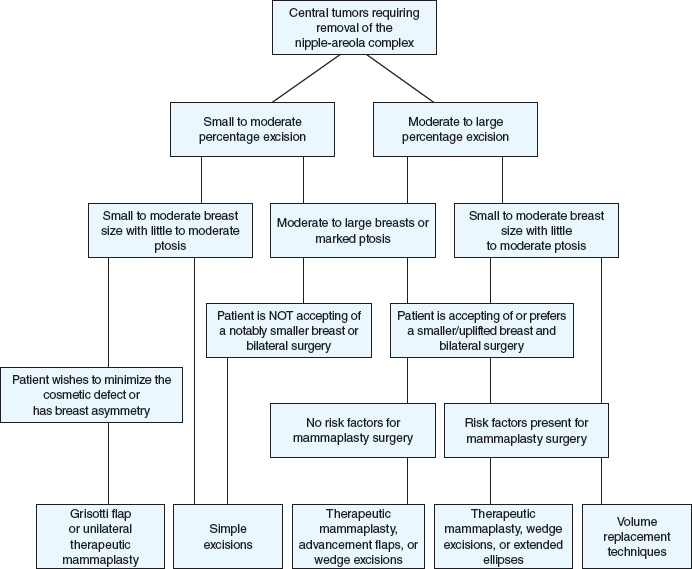
Important influences on the technique selection include degree of ptosis, breast size, any preexisting breast asymmetry, surgical risk factors, the desired margin of excision, the patient’s preferences regarding breast size and willingness to undergo bilateral surgery, and to a lesser degree, her age. All of these factors need to be considered when discussing the options with the patient.
Therapeutic mammaplasty is our preferred term for the use of mammaplasty techniques for the primary treatment of breast tumors. It is an ideal option for women at risk of deformity after breast-conserving surgery (BCS), especially if they consider an uplifted or smaller breast to be a positive outcome.
For central tumors the surgical options include simple or modified ellipse excisions, round bloc purse-string excisions, therapeutic mammaplasty, and volume replacement techniques. Therapeutic mammoplasty can again be divided into either a reduction mammaplasty when significant volume is removed or mastopexy mammaplasty when the only volume excision is the wide local excision. For very large–breasted patients, almost regardless of the tumor size, the advantages of a smaller breast with regard to postoperative radiotherapy should be emphasized. 5 , 6 For suitable cases, mammaplasty surgery is particularly safe and reliable, because there is no requirement for a pedicle to the nipple. In many situations, a nipple reconstruction can be performed primarily. This may be on a skin-bearing inferior pedicle with a mammoplasty, 3 , 7 a skin-bearing local perforator flap, or may be performed on the remaining local skin after nipple areolar excision.
When bilateral surgery is neither favored by the patient nor thought to be required by the surgeon, unilateral surgery should be performed. Small excisions can be treated with simple ellipse excisions or Grisotti flap techniques. Larger excisions (those involving more than 15% of the breast volume) can be treated with a unilateral extended ellipse, a Grisotti flap, or a unilateral therapeutic mammaplasty. When there is insufficient ptosis or volume to consider a mammaplasty or no change in breast volume is required, volume replacement techniques are preferable. These are particularly used in the smaller breast.
Surgical Techniques
Box 17-1 Surgical Options for Centrally Located Tumors
Simple excisions
Central ellipse
Round block
Volume displacement techniques
Therapeutic mammaplasty wedge excisions
Therapeutic mammaplasty with parenchymal advancement
Grisotti flap
Therapeutic mammaplasty with parenchymal flaps
Volume replacement procedures
Simple Excisions
Central Ellipse
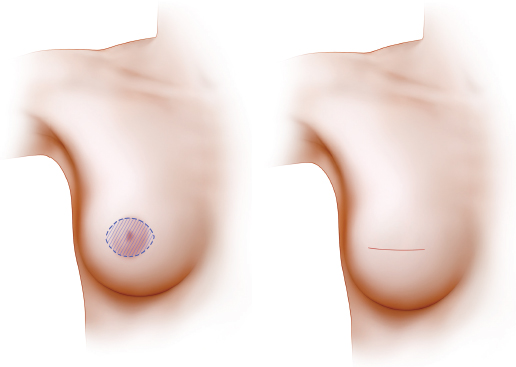
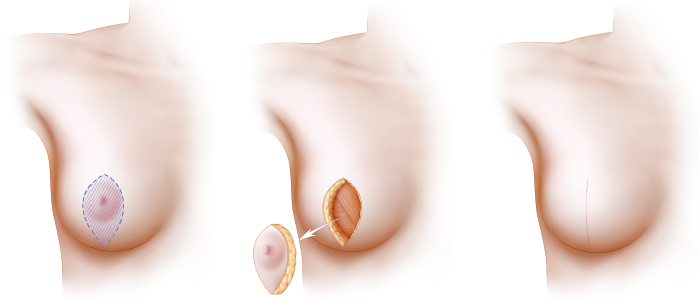
Ellipse excisions are easy to perform, but they always flatten the breast apex, resulting in some asymmetry. Little or no skin undermining is required. This is a good option when a small volume is to be excised and/or a limited surgery is favored, regardless of the breast size or shape. Ellipse excisions are usually transversely oriented, but they may be rotated if necessary and are performed as a single excision of cutaneous and parenchymal tissue.
The wider the ellipse excision of the skin and areola, the greater the breast flattening. This effect can be limited by narrowing and shortening the excision.
One method of decreasing flattening is to remove the nipple and leave some areola, if oncologically feasible. In addition to limiting the flattening effect, the remaining areolar tissue may also add to the cosmetic outcome.
Alternatively, the ellipse may be made in a vertical direction with the superior extension limited. In principle, this becomes a vertical wedge mammaplasty, but it is almost as easy to perform as a horizontal ellipse. The vertical orientation tends to tighten or lift the breast and can often be performed in conjunction with a vertical mastopexy on the opposite breast. It is ideal in breasts with minor to moderate ptosis. As with the transverse ellipse, it is not necessary to remove all of the areola with this method.
An extended ellipse, or melon slice excision is usually performed transversely but can be at an oblique angle if required. It is a simple method of simultaneously excising the tumor and nipple-areola complex and significantly reducing the breast size. It is a helpful technique if a wide margin is preferred, in reexcision cases, in patients with risk factors, in elderly patients for whom a quick, simple procedure may be preferable, and if the patient prefers a smaller breast or this facilitates postoperative radiotherapy.
Therapeutic mammaplasty achieves similar goals but is more complex. An extended central ellipse is preferred for patients with risk factors, since there is very little undermining of breast tissue or pillar creation as for mammaplasty surgery, minimizing the healing risks for patients who smoke, are obese, have diabetes, or those with very soft, oily parenchymal tissue.
Although the disadvantage of an extended ellipse is a long, transverse scar across the breast, the advantages include its simplicity, relative safety, and predictability. Preoperative markings are essential. The tumor is best marked with the patient lying down; the mammaplasty marks should be made with the patient standing. The resection needs to extend across the entire breast to minimize contour irregularities. The superior marking of the ellipse is placed at or just below the IMF and then a gentle curve is drawn medially to a chosen point on the medialmost aspect of the breast. The ellipse is concave inferiorly. The lateral markings should have a slightly wider or higher marking to create a somewhat wider excision laterally. This helps to narrow the breast. The inferior marking of the ellipse needs to retain 8 to 14 cm of central tissue above the IMF to create enough central bulk for the breast. At the breast meridian the ellipse is convex superiorly. It is possible to leave some additional tissue on either the superior or inferior aspect of the ellipse, depending on the tumor excision site. The tumor is excised first, and then the remaining excision and axillary surgery are performed. The superficial fascia is reapproximated to lift the breast and close the dead space.
Patient Example

This 52-year-old woman was diagnosed with a screening-detected invasive tumor in her left breast that measured 33 mm on imaging and required excision of the nipple-areola complex. It is important to note that the patient is overweight and diabetic. A left extended ellipse and a right Wise pattern reduction were performed. The patient is shown 4 months after surgery and radiotherapy.
Round Block
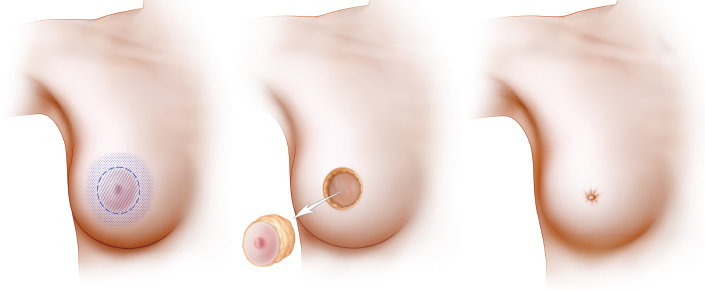
The round block excision with a purse-string closure is an attractive option, because it results in a reduced scar length. The nipple and areola are excised with the underlying tumor, and the skin surrounding the excision is undermined. The parenchyma is approximated, and the skin is closed with a purse-string suture. However, although the scar is shorter, this technique also produces flattening of the breast apex, and the scar has a tendency to stretch and is prone to healing problems. It is not always ideal for nipple reconstruction. However, this round block excision remains a simple option for small, unilateral cases.
Volume Displacement Techniques
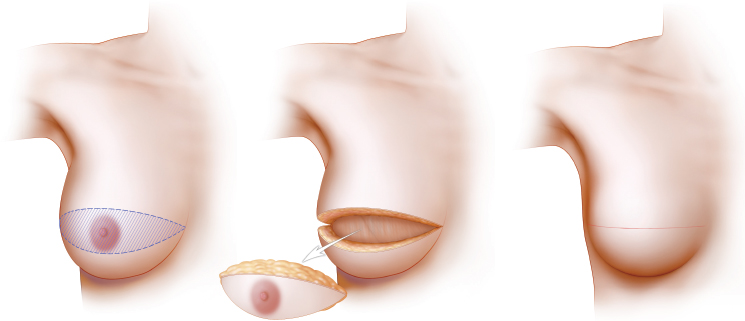
Because of the relative simplicity of planning mammaplasty surgery in which the nipple-areola complex is to be excised, therapeutic mammaplasty is a very useful and reliable tool in patients with central tumors. Although modifications are required in mammaplasty techniques when applied to tumors throughout the breast, central tumors may be treated by one of two therapeutic mammaplasty methods. The first and simpler method is the wedge excision, in which the central tumor, nipple, and additional tissue are removed as required. These incisions are usually in the form of a vertical or inverted-T skin pattern. No pedicles are required for the nipple or to fill in the tumor defect. This simplifies the surgery and reduces the risk of complications.
The second group of techniques for central tumors uses an inferiorly based pedicle to fill the parenchymal and nipple-areola defect. A central skin island is created to replace the nipple-areola complex. The surgery is usually bilateral. These procedures are broadly based on the principles of the Grisotti flap, using an inferior pedicle that advances or rotates into the central defect.
Therapeutic Mammaplasty Wedge Excisions
Of all the therapeutic mammaplasty options, a wedge mammaplasty excision remains one of the easiest to perform; it is also ideal for managing central tumors in which the nipple-areola complex is to be removed.
It is usually planned as either a vertical or inverted-T pattern. The skin pattern is determined by the size of the breast and the degree of ptosis.
Because no pedicles are used, wedge excisions are a predictable procedure for patients with extremely large breasts or risk factors such as obesity, smoking, or diabetes. These procedures are ideal as a primary excision and in reexcision cases.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


