22 Pedicled Perforator Flap Reconstruction
Breast-conserving therapy (BCT), a combination of tumor resection and postoperative radiotherapy, has become the preferred treatment for early stage invasive breast cancer. 1 – 3 Although partial mastectomies (lumpectomy or quadrantectomy) conserve the nipple-areola complex, 20% to 30% of patients are dissatisfied with the aesthetic result after BCT. 4 – 7 There are many possible causes of aesthetic failure. The tumor resection can produce distortion, retraction, and noticeable volume changes in the breast. Changes to the position of the nipple-areola complex can accentuate asymmetry. Radiation can also have a profound effect on the breast. Initially, radiation causes generalized breast edema and skin erythema. Long-term effects of radiation to the breast skin include hyperpigmentation, hypopigmentation, telangiectasia, and atrophy. In the breast parenchyma, radiation causes fibrosis and retraction. For most patients, radiation-induced changes plateau 1 to 3 years after treatment. Unfortunately, it is difficult to predict which individuals will develop the most severe postradiation changes. 7 – 9
Most of the poor outcomes result from one of the significant surgical dilemmas that are related to breast cancer treatment—choosing between making wider excisions to attain clear margins and better local control of the disease and sparing as much breast tissue as possible to adequately close the defect and optimize the aesthetic outcome. 10 , 11 Therefore we prefer to perform immediate reconstruction whenever it is indicated and feasible, because operating on irradiated breasts has high complication rates with frequently poor aesthetic results. In small- to moderate-sized breasts, tissue replacement techniques using pedicled flaps are required to restore the breast shape and size. Although the thoracodorsal and intercostal vessels provide many perforators to the region of the back, only the latissimus dorsi flap is described for partial breast reconstruction; it requires sacrificing the largest muscle in the body. As the perforator flap concept has gained acceptance, many previously described myocutaneous flaps have been harvested as perforator flaps. Harvesting the flap without sacrificing the muscle or nerve is essential in this technique.
Therefore the donor-site morbidity is reduced to the absolute minimum. In 1995 Angrigiani et al 12 first described the use of a cutaneous island of the latissimus dorsi flap without the muscle based on one thoracodorsal cutaneous perforator as a free flap transferred for cervical burn contracture. However, the use of pedicled perforator flaps in partial breast reconstruction is a relatively new concept and it was first described by Hamdi et al. 13 – 17 Nevertheless, they have become an integral part of the armamentarium of oncoplastic techniques available for partial breast reconstruction.
Decision-Making Process
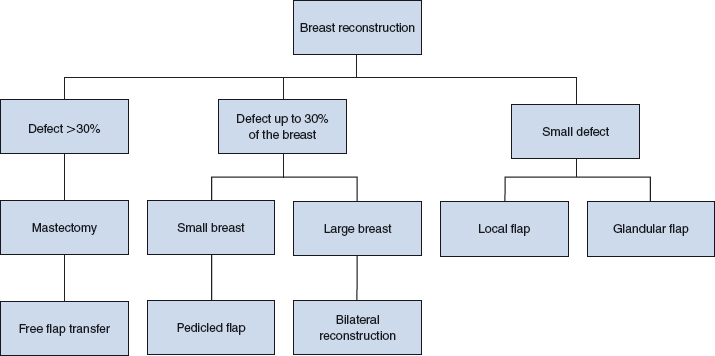
The ultimate goal when using pedicled perforator flaps in oncoplastic surgery is to reduce donor-site morbidity. 18 The major indications for this flap are defects estimated to be up to 30% of the breast size, or any case in which the tumor resection will result in an unacceptable aesthetic result. 19 , 20 The clinical application of pedicled perforator flaps in partial breast reconstruction is based on a combination of factors.
Factors Related to the Tumor
As for any conservative breast therapy, the safest treatment for tumors up to 3 cm in diameter is a quadrantectomy with postoperative radiotherapy; mastectomy is still the first choice for larger tumors. However, the introduction of more efficient protocols of neoadjuvant chemotherapy may allow a more conservative local approach to advanced tumors. 21 – 22
Any immediate partial reconstruction should be delayed if the surgeon is uncertain about the margins or tumor extension, despite the preoperative radiologic assessment. A delayed-immediate reconstruction can still be performed within a few days after the definitive margin status is known. 23
Factors Related to the Size of the Breast
Many surgeons have suggested incorporating a reduction mammaplasty–type procedure during the tumor resection in patients with large breasts. 16 – 21 However, one of the relative anatomic contraindications for rearrangement breast surgery is a large tumor/breast ratio. Smaller breasts require different methods of reconstruction. If a significant postoperative deformity is expected because of a large-volume tumor resection in a smaller breast, the recruitment of nonbreast tissue is required. Depending on the location and the size of the breast defect, a variety of pedicled perforator flaps can be used for partial mastectomy reconstruction. 13 , 19 , 20 , 24
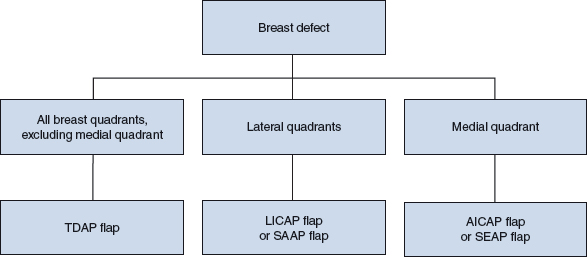
Factors Related to the Location of the Defect
Almost all postquadrantectomy defects can be reconstructed with a pedicled perforator flap. However, depending on the pedicle length, some flaps are more suitable for certain defects. Defects located at the inferomedial quadrant of the breast are difficult to reach using a pedicled perforator flap raised on the thoracodorsal or intercostal vascular pedicle axis. However, some defects can still be considered for reconstruction with pedicled flaps based on the anterior thoracic vessels, such as the intercostal or superior epigastric vessels. 15 , 17
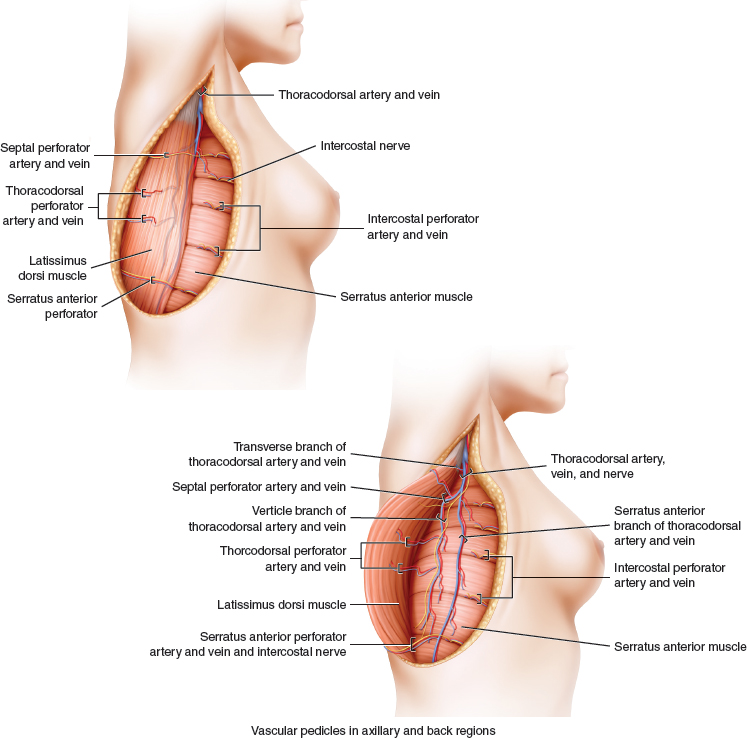
Based on the thoracodorsal-serratus, intercostal, or superior epigastric vessels, several pedicled flaps can be raised on perforators, either in the axillary and back regions or the anterior thoracic and upper abdominal regions.
The pedicled perforator flaps commonly used for breast reconstruction are the thoracodorsal artery perforator (TDAP) flap, the intercostal artery perforator (ICAP) flap, the serratus anterior artery perforator (SAAP) flap, and the superior epigastric artery perforator (SEAP) flap.
TDAP flap
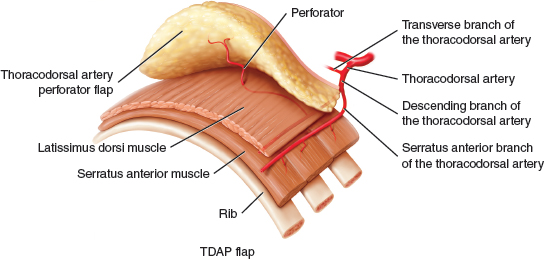
The TDAP flap is based on perforators raised from the descending or horizontal branches of the thoracodorsal vessels. 22 , 25 However, a segment of latissimus dorsi muscle can be included in the flap because of anatomic variations, thus creating one of the types of muscle-sparing latissimus dorsi TDAP flaps described in the following text 13 , 16 :
Muscle-sparing latissimus dorsi TDAP I flap: A small piece of latissimus dorsi muscle (4 cm by 2 cm) is incorporated in the flap.
Muscle-sparing latissimus dorsi TDAP II flap: A larger segment (up to 5 cm wide) is designed along the anterior border of the latissimus dorsi muscle.
ICAP flap
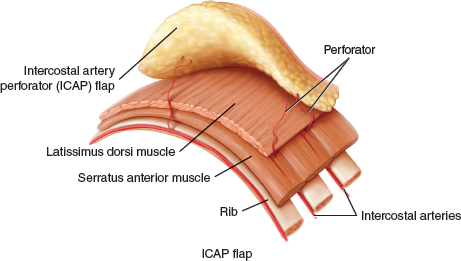
The ICAP flaps are classified as follows 14 :
Dorsal intercostal artery perforator (DICAP) flap. The flap is based on perforators arising from the vertebral segment of the intercostal vessels.
Lateral intercostal artery perforator (LICAP) flap. The flap is based on perforators originating from the costal segment.
Anterior intercostal artery perforator (AICAP) flap. The flap is based on perforators originating from the muscular segment.
SAAP Flap
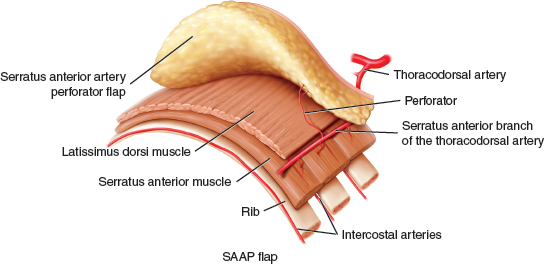
The SAAP flap is based on the connection between the serratus branch of the thoracodorsal artery and the intercostal perforators. This connection is found in 21% of cases. 17
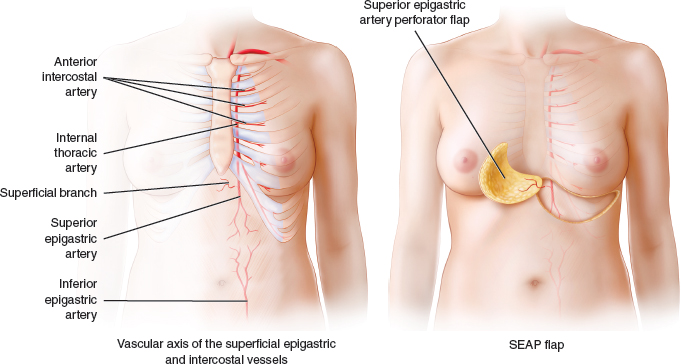
The SEAP flaps are based on perforators originating from either the superficial or the deep branch of the superior epigastric artery and are classified as follows 15 :
Superficial superior epigastric artery perforator (SSEAP) flap
Deep superior epigastric artery perforator (DSEAP) flap
Preoperative Planning
The patient is marked the day before surgery. The incision of the tumor resection is planned with the breast surgeon to provide the best access for resection and the best aesthetic result.
Preoperative Perforator Mapping
It is essential to locate the perforators preoperatively. Careful perforator mapping is a decisive step for choosing a pedicled perforator flap and reduces the operative time and complication rate significantly. Unidirectional Doppler (8 Hz) ultrasonography is used to locate potential perforators on which the flap is designed. Based on previous anatomic studies and our clinical experience, 16 , 25 we look for perforators in a region 8 to 10 cm below the axillary crease and within 5 cm of the anterior border of the latissimus dorsi muscle.
A possible pitfall of using unidirectional Doppler ultrasonography to identify the thoracodorsal perforators is the background signal from the main thoracodorsal pedicle. To avoid this, the patient is positioned for perforator marking in the same position she will be in during surgery—a lateral decubitus position with 90 degrees of shoulder abduction and 90 degrees of elbow flexion.
This positioning places the skin under tension, causing the perforators to enter the skin with a more perpendicular orientation, which makes their Doppler signal more distinct. In this orientation, the Doppler unit detects the signal from the discrete end of the perforator rather than along its length. This allows one to differentiate between the signal from the perforator and the longitudinally oriented thoracodorsal pedicle. True perforator tones can be distinguished from the thoracodorsal artery by moving the Doppler probe proximally and distally. If the signal disappears, it belongs to a perforator; signals from the thoracodorsal vessels are present continuously along the length of the latissimus dorsi muscle. When the perforator is located in front of the anterior border of the latissimus dorsi muscle, a direct (septal) perforator from the thoracodorsal artery can be expected.
Intercostal or superior epigastric perforators are mapped while the patient is in the supine position. In difficult cases, a duplex examination is performed. 26 More recently, the multidetector CT has been introduced to preoperatively localize various perforators. 27 – 29
Defects Located in the Lateral, Superolateral, or Superomedial Quadrants
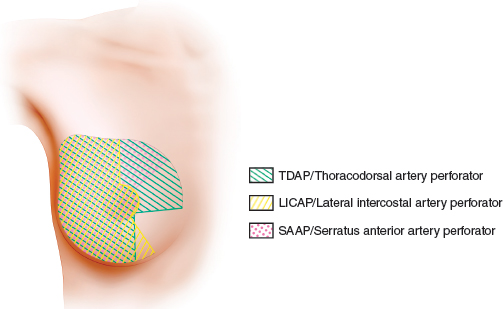
Defects located in the lateral, superolateral, or superomedial quadrants are usually reconstructed with either the TDAP or the LICAP flap. The skin marking begins with the patient in an upright position. The anterior border of the latissimus dorsi muscle is palpated and marked. The patient is asked to lie down on her side, similar to the intraoperative position. The width of the TDAP flap is determined based on the expected breast defect and the possibility for primary donor-site closure. The excess of skin and fat of the back is determined using the pinch test. The average flap size is 20 by 8 cm (range 16 to 25 cm long and 6 to 10 cm wide). The flap paddle is oriented parallel to the skin lines. The island can also be horizontally designed, according to the wishes of the patient. It is always extended over the anterior border of the latissimus dorsi muscle to include the premuscular perforators, if they can be found. The length of the skin paddle depends on the location of the defect. When the defect is located in the lateral or superolateral quadrants, the skin paddle is designed over the lateral thoracic area. The proximal edge of the flap reaches the inframammary fold. For more medially located defects, the skin paddle is designed more distally, toward the back.
Patient Examples
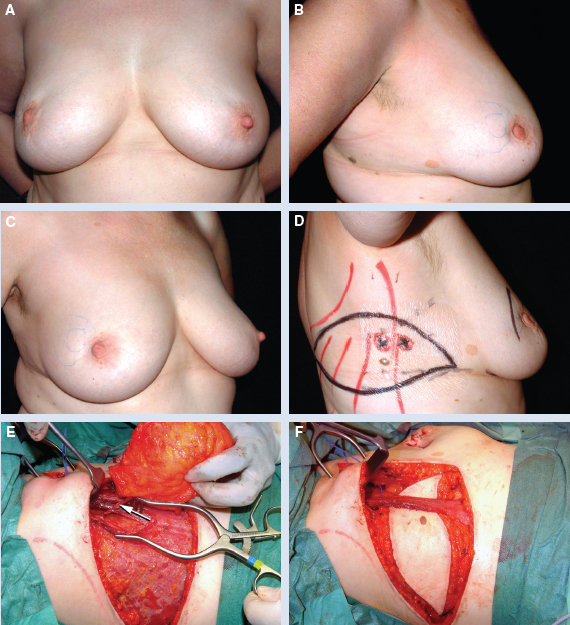
This 53-year-old patient had a tumor (invasive ductal carcinoma) located in the right superolateral quadrant (A through C). A pedicled (21 by 8 cm) TDAP flap was designed with a horizontal orientation over the lateral thoracic region, with two perforators detected using a unidirectional Doppler probe (D). The intraoperative view shows the dissection of one perforator (arrow) through the split latissimus dorsi muscle (E). The thoracodorsal nerve branches to the latissimus dorsi muscle were spared. The flap was passed through the split latissimus dorsi muscle (F).
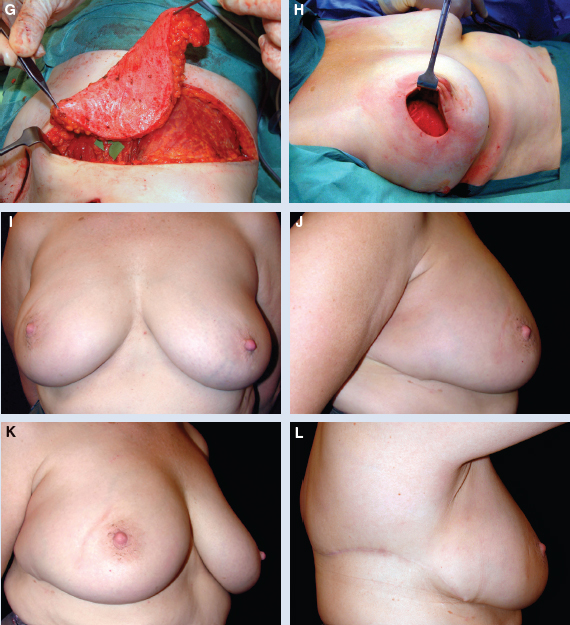
The flap was completely deepithelialized (G). The flap was set into the postquadrantectomy defect (specimen weight 98 g) (H). The patient is shown 18 months postoperatively (I through K). The donor site also is shown 18 months postoperatively (L).
The LICAP flap is designed in a similar way. According to our anatomic study, 17 the largest perforators that may be used for breast surgery are located between the fourth and sixth intercostal spaces. Their distances to the anterior border of the latissimus dorsi muscle are between 0.8 and 3 cm. Therefore they are more suitable for defects in the lateral and inferior quadrants. The flap is designed over the lateral thoracic region at the level of the inframammary fold.
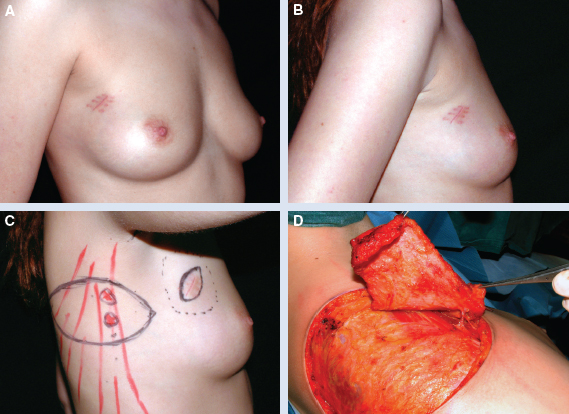
This 32-year-old patient has already had a tumor excised (invasive ductal carcinoma) from the superolateral quadrant of the right breast (A and B). The margins were involved, and the patient was scheduled for further excision. The breast size was small, and any further excision without reconstruction would result in a major breast deformity. Partial breast reconstruction with a pedicled perforator flap was planned. The flap was designed to include the perforators located very close to the anterior border of the latissimus dorsi muscle (C). The flap was raised on an intercostal perforator without jeopardizing the latissimus dorsi muscle or its blood supply (D).
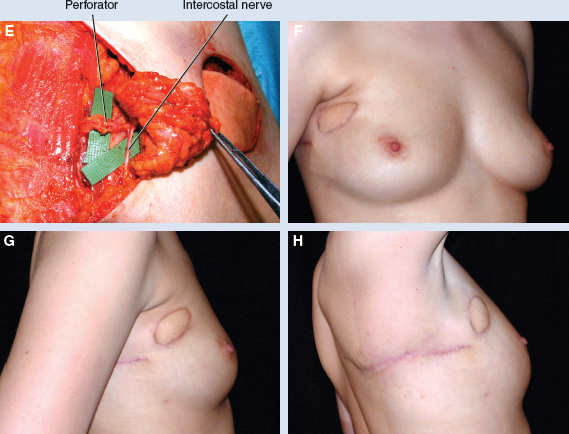
The flap was rotated 180 degrees to fill the defect (E). The patient is shown postoperatively (F and G). The donor site also is shown postoperatively (H). Raising an SAAP flap can only be performed when the vascular connection between the serratus branch and an intercostal perforator is found intraoperatively. The flap can reach the superior and inferior lateral quadrants.
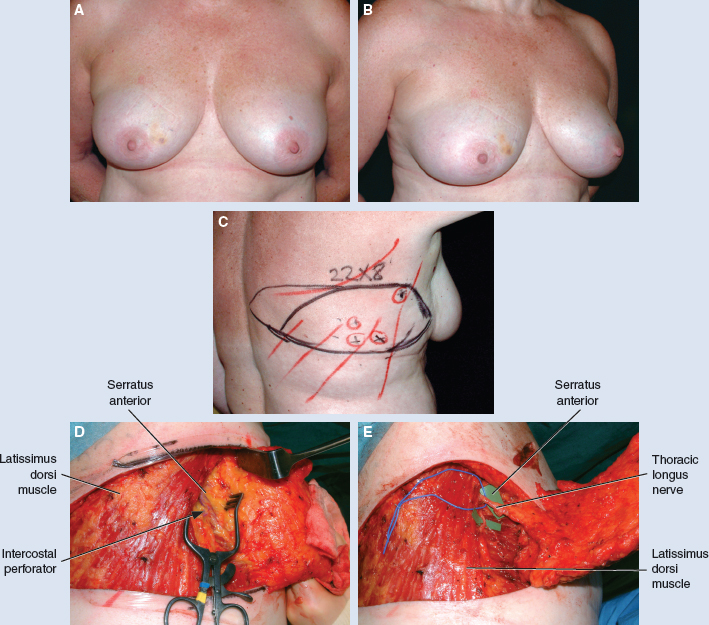
This 65-year-old patient underwent a partial right breast reconstruction with a pedicled SAAP flap (A and B). A 22 by 8 cm flap was designed and the perforators were marked (C). The flap was based on the communication between the serratus anterior muscle and the intercostal perforator (arrow) (D). The connection between the intercostal perforator and serratus anterior muscle was clipped and the flap harvested, based on the serratus anterior vessels and without sacrificing the motor nerve (E).
The patient is shown postoperatively (F and G). The donor site also is shown postoperatively (H).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


