20 Thyroid Eye Disease
Abstract
“Thyroid Eye Disease” discusses the the most common orbital inflammatory disorder and the most common cause of unilateral or bilateral proptosis in adults. Although it was described by Graves in 1835, the disorder remains an enigma, with many major issues remaining unresolved. Known by a variety of terms over the years—Graves’ orbitopathy, Graves’ eye disease, Graves’ ophthalmopathy, thyroid-associated ophthalmology, thyroid exophthalmos, thyroid-related eye disease, and Von Basedow’s ophthalmopathy—it is a very variable disorder with a wide spectrum of clinical presentation, which can result in initial misdiagnosis. Diagnostic accuracy has been improved by advances in both laboratory investigations and orbital imaging techniques. Research continues to improve understanding of the underlying pathogenesis of the disorder. The clinical management of patients has also been greatly improved over recent years with medical advances and with a better understanding of the pathophysiology of eyelid retraction, restrictive myopathy, and compressive optic neuropathy. The surgical approaches to orbital decompression continue to evolve.
20.1 Introduction
Thyroid eye disease is the most common orbital inflammatory disorder and the most common cause of unilateral or bilateral proptosis in adults. Although it was described by Graves in 1835, the disorder remains an enigma, with many major issues remaining unresolved. Over the years it has been known by a number of different terms: Graves’ orbitopathy, Graves’ eye disease, Graves’ ophthalmopathy, thyroid-associated ophthalmology (TAO), thyroid exophthalmos, thyroid-related eye disease, and Von Basedow’s ophthalmopathy.
It is a very variable disorder with a wide spectrum of clinical presentation, which can result in initial misdiagnosis. Diagnostic accuracy has been improved by advances both in laboratory investigations and orbital imaging techniques. Research continues to improve understanding of the underlying pathogenesis of the disorder. The clinical management of patients has also been greatly improved over recent years with medical advances and with a better understanding of the pathophysiology of eyelid retraction, restrictive myopathy, and compressive optic neuropathy (CON). The surgical approaches to orbital decompression continue to evolve.
20.2 Pathogenesis
Although precisely what triggers thyroid eye disease and why the disease is more severe in some patients than others is unknown, the orbitopathy and dysthyroid state appear to be associated with immunological abnormalities. It is generally believed that the orbitopathy may be a closely related but separate organ-specific autoimmune disorder with target autoantigens and circulating autoantibodies.
20.3 Thyroid Orbit Relationship
Approximately 80% of thyroid eye disease cases occur in association with hyperthyroidism, although not all of these coincide with the onset of hyperthyroid symptoms. Patients may present with thyroid eye disease well before the onset of thyroid dysfunction, at the same time as the onset of thyroid dysfunction, or when the patient has become euthyroid after treatment.
When patients who are thought to have euthyroid thyroid eye disease are evaluated more extensively, they are often found to have some features of thyroid disease, such as a positive family history, thyroid stimulating hormone (TSH)–receptor–stimulating antibodies, positive thyroid peroxidase (TPO) antibodies, or an abnormal response to thyrotropin-releasing hormone (TRH). Approximately 50% of the patients with thyroid eye disease who initially appear euthyroid will go on to develop hyperthyroidism within 18 months of presentation.
In addition, approximately 10% of patients with thyroid eye disease have primary autoimmune hypothyroidism. These patients are characterized by the presence of moderate to high titers of TPO antibodies. The orbitopathy in these patients can be as great, or occasionally greater, than that seen in patients with hyperthyroidism.
Men and older patients (older than 50 years of age) tend to have much more aggressive disease. Older patients are also more likely to have unilateral or very asymmetrical disease and are more likely to appear euthyroid or hypothyroid at the time of presentation.
20.3.1 Pathology
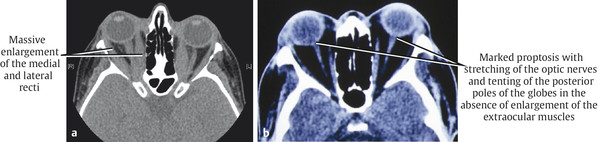
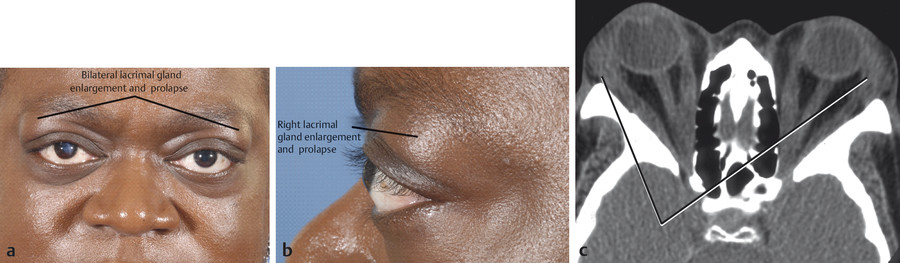
The extraocular muscles show inflammatory cell infiltration with lymphocytes, plasma cells, and mast cells. Although the inferior and medial rectus muscles are more commonly affected clinically, orbital imaging demonstrates that most if not all the extraocular muscles, including the levator muscle, are involved in the disease process. The muscles undergo degenerative changes caused by the deposition of glycosaminoglycans and collagen formation and demonstrate infiltration with fat. The muscle belly is mainly involved in the process, with the muscle tendon showing minimal or no enlargement. This differentiates thyroid eye disease from orbital myositis. The enlarged muscles may reach two to three times their normal volume (Fig. 20‑1a). In most patients, the disease process becomes inactive after a period of 18 months to 2 years. The degenerated extraocular muscles are replaced by fat and fibrous tissue, resulting in a restrictive myopathy in severe or untreated cases.
In most patients, the orbital fat does not undergo significant structural changes, although in some patients the orbital fat has marked volumetric alterations that can be responsible for marked proptosis, even in the absence of extraocular muscle enlargement, as seen on orbital imaging (Fig. 20‑1b).
20.3.2 Pathophysiology
A single extraocular muscle or multiple extraocular muscles may be affected by the disorder. The disorder may present symmetrically or asymmetrically for reasons that are thus far unclear. The extraocular muscle enlargement and/or orbital fat hypertrophy cause a secondary mass effect within the confines of the bony orbit. The secondary effects depend on a number of variable and interacting factors that are responsible for the wide range of clinical presentation of thyroid eye disease. These include the following:
The volume of the orbital cavity.
The axial length of the globe.
The integrity of the orbital septum.
The degree and rapidity of onset of the orbital inflammation.
The degree of enlargement of the extraocular muscles.
The degree of hypertrophy of the orbital fat.
The absence of lymphatics from the posterior orbital tissues.
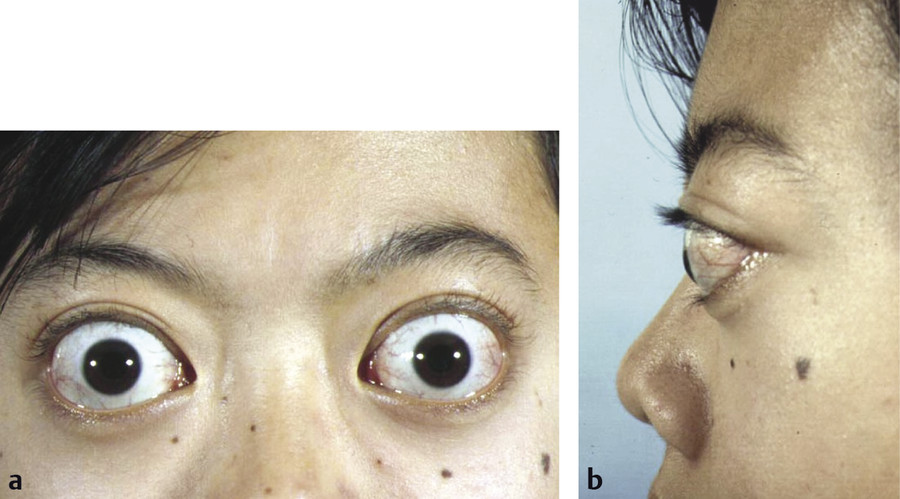
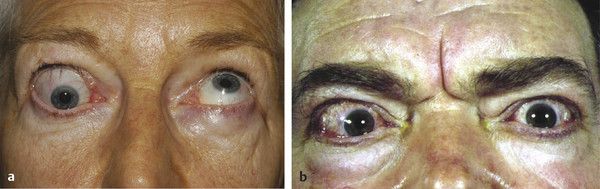
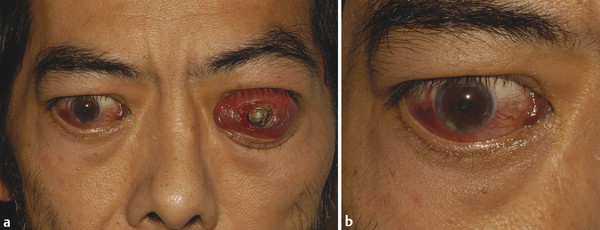
If the orbital cavity is small, any mass effect can result in more severe degrees of proptosis and even in frank subluxation of the globe. This is typically seen in black or Southeast Asian patients. Patients with axial myopia also tend to experience a more severe cosmetic deformity resulting from proptosis (Fig. 20‑2).
The degree of proptosis, which results from the orbital mass effect, is influenced by the tightness of the orbital septum. A lax orbital septum offers little resistance to the forward movement of the globe. The degree of resultant proptosis is governed by the size of the orbital cavity, the axial length of the globe, the degree of extraocular muscle and/or orbital fat swelling, the compliance of the extraocular muscles, and the length of the optic nerve. The resultant proptosis represents a spontaneous orbital decompression that may be severe enough to result in spontaneous subluxation of the globe. It may also be severe enough to cause a stretching of the optic nerve and deformation of the posterior aspect of the globe that may cause an optic neuropathy with visual loss.
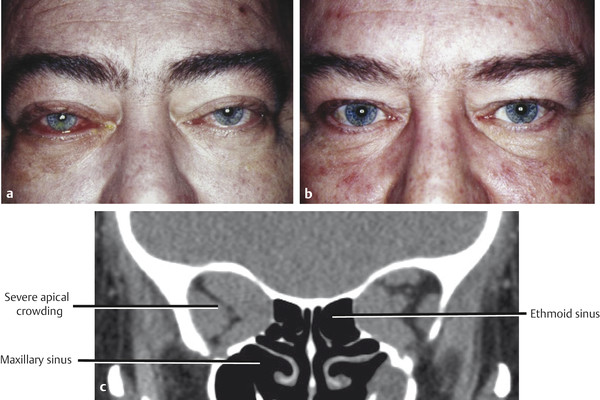
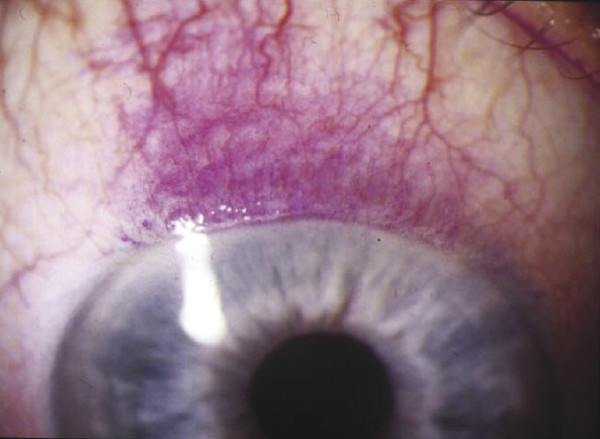
In contrast, if the orbital septum is tight, as seen in younger patients, the globe is prevented from moving forward and the pressure within the orbit rises. This rise in intraorbital pressure, in conjunction with swelling of the extraocular muscles in the confined bony space of the orbital apex, can result in an insidious compressive optic neuropathy (CON). The degree of visual impairment may be out of proportion to the apparent clinical extent of the disease (Fig. 20‑3).
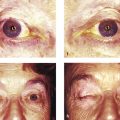
The tightness of the orbital septum and the absence of deep orbital lymphatic vessels also influence the magnitude of secondary periorbital tissue edema. If the orbital inflammation progresses rapidly, the secondary congestive changes can be severe, resulting in so-called “malignant exophthalmos” (Fig. 20‑16).
20.3.3 Epidemiology
The estimated incidence of thyroid eye disease in the general population is 16 females and 3 men per 100,000 population annually. The prevalence appears to have declined in most European countries over the last decade, a trend that may be related to earlier diagnosis and management of thyroid dysfunction by endocrinologists and a decreased prevalence of smoking. It is well recognized that smoking greatly increases the severity of the ophthalmopathy.
Patients with thyroid eye disease tend to be older than patients presenting with Graves’ hyperthyroidism. The disease is more common in women than men, but men tend to have a more severe ophthalmopathy, as do older patients. Patients of European descent have a far greater risk of developing thyroid eye disease than those of Asian descent.
A number of factors may increase the risk of developing thyroid eye disease in patients with Graves’ disease. These include genetic predisposition, gender, radioactive iodine treatment, smoking, TSH-receptor antibodies, drugs, age, and stress.
Patients often have a history or family history of other autoimmune disorders, such as type 1 diabetes mellitus, pernicious anemia, rheumatoid arthritis, Addison’s disease, and myasthenia gravis. The prevalence of insulin-dependent diabetes mellitus is higher in patients with thyroid eye disease than in the normal population. Also, patients with thyroid eye disease and diabetes have a higher incidence of CON and have a worse recovery of visual function after treatment of the neuropathy. These patients also pose a higher risk of intraoperative and postoperative bleeding.
Myasthenia is 50 times more common in patients with thyroid eye disease compared with the general population. Patients with thyroid eye disease who develop ptosis or a changing pattern of ocular motility restriction should be investigated for myasthenia.
Key Point
Patients with thyroid eye disease who develop ptosis or a changing pattern of ocular motility restriction should be investigated for myasthenia.
20.3.4 Clinical Presentation
The clinical manifestations of thyroid eye disease can be very variable and may be acute or insidious in onset. Patients can be divided into two subtypes.
Type 1
Patients with type 1, or “noninfiltrative,” orbitopathy tend to be younger and usually present with symmetrical proptosis, eyelid retraction, minimal inflammatory signs, and no extraocular muscle restrictions (Fig. 20‑4). These clinical features tend to be manifestations of hyperthyroidism and may even regress once the hyperthyroidism has been controlled. The diagnosis of thyroid eye disease in this subset of patients does not usually present a problem.

Type 2
Patients with type 2 or “infiltrative” orbitopathy are usually middle-aged and run a much more fulminant course. The orbitopathy is likely to be more asymmetrical, and the patient is likely to present with chemosis, diplopia, and CON (Fig. 20‑5).

20.3.5 Clinical Symptoms
The symptoms of thyroid eye disease are variable and may be nonspecific. They include ocular irritation, a foreign body sensation, tearing, photophobia, diplopia, and visual impairment. Diplopia, when it develops, is usually first noticed either on waking, when tired, or on extremes of gaze. It is sometimes accompanied by aching, particularly on upgaze. Some patients with type 2 orbitopathy complain of a constant deep boring orbital pain unrelated to ocular movements.
Visual complaints such as blurring of vision, which may be patchy or generalized, or disturbances of color perception occur in only 5% of patients. These complaints may, however, herald the onset of CON, and because the symptoms may not be volunteered by the patient, they should be specifically elicited in the history in all patients.
Patients are also greatly disturbed by changes in their appearance caused by the disease process. Subluxation of the globe is very rare but can be extremely alarming and upsetting for both the patient and witnesses to the event. It is more likely to affect patients with shallow orbits, such as are common in black patients.
20.3.6 Clinical Signs
The physical signs are variable, and it is very unusual for a patient to present with all of them. The physical signs include the following:
Proptosis.
Eyelid retraction.
Eyelid lag.
Lagophthalmos.
Periorbital edema.
Conjunctival and caruncular edema.
Eyelid erythema.
Injection of the vessels along the horizontal recti.
Limitation of ocular motility.
Exposure keratopathy.
Glabellar rhytids.
Superior limbic keratoconjunctivitis.
Optic disc edema or pallor with signs of optic nerve dysfunction.
Raised intraocular pressure on attempted upgaze.
Choroidal folds.
Globe subluxation.
Lacrimal gland enlargement or prolapse.
It should be noted that these physical signs, with the exception of superior limbic keratoconjunctivitis and glabellar rhytids, may be observed, singly or in combination, in any orbital inflammatory disorder, although upper lid retraction with lid lag is more typical in patients with thyroid eye disease.
Key Point
The main physical signs seen in thyroid eye disease may be observed, singly or in combination, in any orbital inflammatory disorder.
The physical signs in thyroid eye disease can alter with subtle remissions and exacerbations.
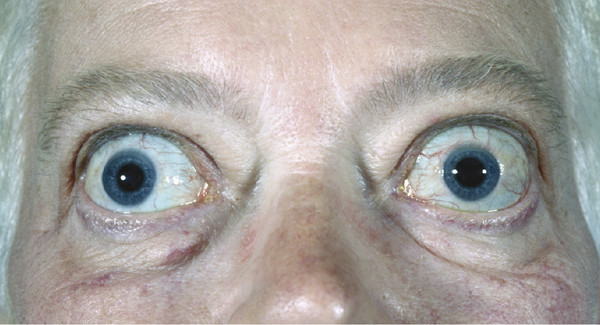
Thyroid eye disease is the most common cause of unilateral or bilateral proptosis in an adult (Fig. 20‑6).
Proptosis correlates significantly with lower lid retraction (Fig. 20‑7). It should be borne in mind, however, that proptosis in a patient with known thyroid dysfunction may have another cause. Patients may have more than one underlying pathological process responsible for their proptosis, particularly when it is asymmetrical.

The causes of eyelid retraction in thyroid eye disease are discussed in Chapter 8. Eyelid retraction is the most common sign seen in thyroid eye disease and affects the vast majority of patients at some stage. It frequently varies with attentive gaze (Kocher’s sign). If eyelid retraction is absent, it is wise to question the diagnosis. Eyelid retraction may often be accompanied by a lateral flare, an appearance that is almost pathognomonic for thyroid eye disease (Fig. 20‑8). The downward movement of the upper eyelid often lags behind the downward movement of the globe and remains high (lid lag or von Graefe’s sign) (Fig. 20‑8b,c). Patients with marked proptosis and eyelid retraction are at risk of incomplete reflex or voluntary eyelid closure (lagophthalmos). This can lead to corneal exposure and sight-threatening corneal ulceration, particularly in patients with an absent Bell’s phenomenon. The keratopathy can be exacerbated in some patients whose proptosis can also result in a lateral upper eyelid entropion (Fig. 20‑8d).
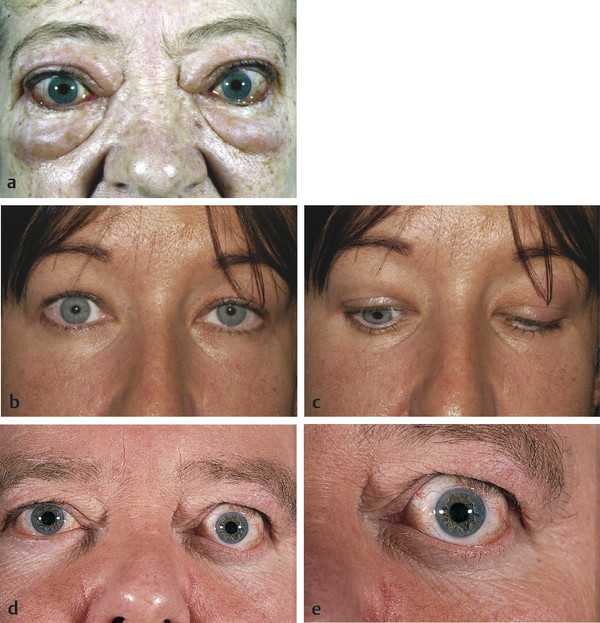
Although ptosis can develop in long-standing thyroid eye disease, usually because of a levator aponeurosis dehiscence secondary to marked upper eyelid edema, it is very unusual for patients to present with a ptosis. The presence of a ptosis should raise the suspicion that the patient has a concomitant ocular myasthenia or myasthenia gravis. Likewise, a divergent strabismus is unusual in thyroid eye disease and should again raise the suspicion of myasthenia (Fig. 20‑6).
Key Point
If upper eyelid retraction is absent, the diagnosis of thyroid eye disease should be questioned.
Periorbital edema is an early sign of thyroid eye disease. The edema is variable and can be particularly prominent in the upper lids and tends to be maximal in the morning, diminishing throughout the day (Fig. 20‑8).
Periorbital edema should be differentiated from eyelid fat prolapses, which patients often refer to as eyelid swellings.
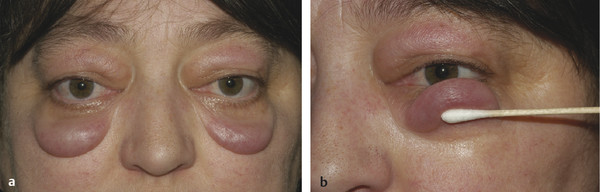
Subcutaneous fluid pouches, referred to as festoons, may occur at the junction of the lower eyelids and cheek (Fig. 20‑9). Occasionally these may persist for many years after the disease has become inactive.
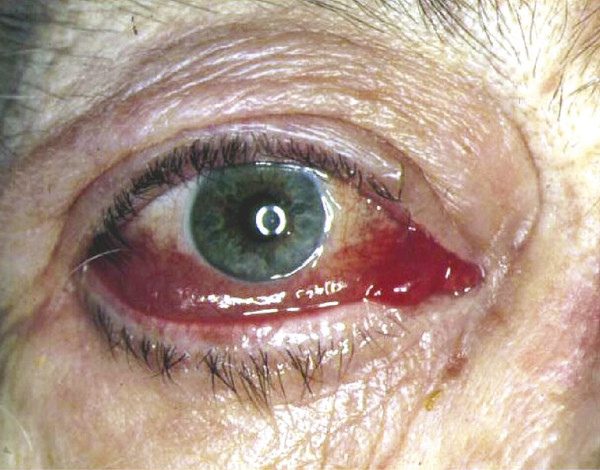
Caruncular edema may be quite subtle. This, in conjunction with conjunctival chemosis, is a clinical measure of disease activity and response to medical therapy. Chemosis can be very marked in some patients and may interfere with the normal distribution of the tear film (Fig. 20‑10). Erythema localized to the eyelids is not uncommon and may persist for many years.
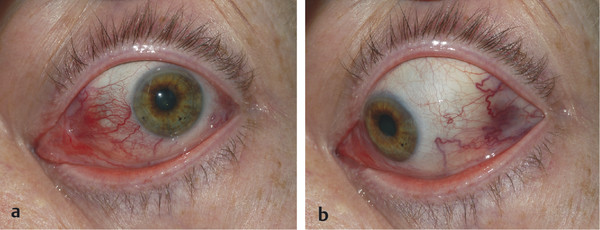
Injection of episcleral vessels occurs along the course of the horizontal recti, which helps to differentiate thyroid eye disease from a local-flow arteriovenous shunt (Fig. 20‑11).
Ocular motility limitation is often variable and commonly asymmetrical (Fig. 20‑12a). Symmetrical restriction may spare the patient from diplopia, but typically asymmetrical progression results in diplopia. The inferior recti followed by the medial recti are the most commonly affected muscles (Fig. 20‑12a,b). Vertical diplopia with discomfort and pain that increases on upgaze is most common. Forced duction testing confirms restriction of motility. A rise in intraocular pressure may be noted on upgaze. It is important not to overlook the possibility of myasthenia gravis as a cause of a changing or unusual ocular deviation in a patient with thyroid eye disease.
Exposure keratopathy can result from the following:
Severe proptosis.
Eyelid retraction with lagophthalmos.
Conjunctival chemosis causing dellen formation.
All corneal signs are secondary phenomena of thyroid eye disease. A widened palpebral aperture results in more rapid tear evaporation, which, in combination with incomplete eyelid closure, results in superficial punctuate erosions and the symptoms of superficial ocular irritation. These symptoms in turn cause the patient to overuse the corrugator supercilii and procerus muscles with the development of marked glabellar rhytids (see Fig. 20‑12b). Corneal thinning, scarring, or frank ulceration can occur, resulting in severe visual morbidity (Fig. 20‑13).
Superior limbic keratoconjunctivitis is a nonspecific ocular lesion that has no known cause but is commonly associated with thyroid eye disease when present bilaterally (Fig. 20‑14).
In patients with a restrictive myopathy, the intraocular pressure (IOP) may rise on attempted upgaze. The diagnosis of primary open angle glaucoma (POAG) should be made with caution for patients with thyroid eye disease, because an increased IOP may simply be the result of a slight elevation of the eyes forced by the head posture required for applanation tonometry. The increase in IOP when looking upward is common in patients with thyroid eye disease, and it does not cause glaucoma more often than in the general population.
CON can occur as an insidious complication of thyroid eye disease, often occurring in patients without marked proptosis and often in the absence of any fundoscopic abnormalities. Only a small percentage of patients demonstrate optic disc edema. The incidence of optic neuropathy in patients with thyroid eye disease is approximately 4 to 5%. A high index of suspicion for its development should be maintained when examining patients with thyroid eye disease. In general patients with a more severe myopathy pose the greatest risk for the development of CON.
Key Point
CON can occur as an insidious complication of thyroid eye disease, often occurring in patients without marked proptosis and often in the absence of any fundoscopic abnormalities. In general patients with a more severe myopathy pose the greatest risk for the development of CON.
Choroidal folds are very rare (Fig. 20‑15). They are believed to develop when the globe is mechanically deformed by the secondary effects of extraocular muscle enlargement in a confined bony space.

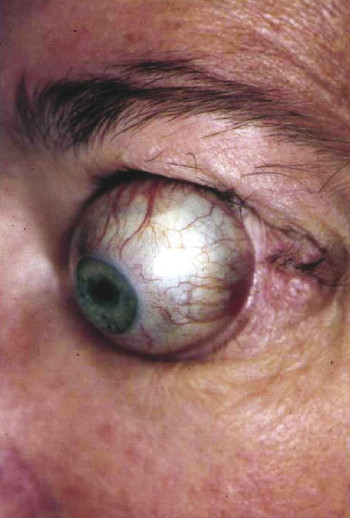
Subluxation of the globe is a distressing situation for a patient where the eyes are so protrusive that they may prolapse out of the orbit, especially on attempting to look up. The eyelids may close behind the eye (Fig. 20‑16). Such patients are naturally reluctant to look up during examination of their ocular motility. Great care should be taken during the use of an exophthalmometer, which can also provoke a globe subluxation. If subluxation occurs the globe should be manually repositioned immediately.
Lacrimal gland enlargement may also be seen in some patients, and, particularly in patients with shallow orbits and extreme degrees of proptosis, the glands may prolapse (Fig. 20‑17).
20.3.7 Patient Evaluation
In most patients with thyroid eye disease, there is no difficulty in establishing the diagnosis, because there is a prior history of thyroid dysfunction or characteristic clinical findings. In patients with no prior history of thyroid dysfunction, thyroid function tests are performed along with antibody studies. The diagnosis can be particularly difficult to establish in the small percentage of patients who present with no prior history of a thyroid disorder or who demonstrate no abnormality of thyroid function. The assistance of an endocrinologist should be sought in the evaluation and management of all patients with suspected thyroid eye disease.
When evaluating a patient referred with thyroid eye disease, it is important to address two initial questions.
Is the diagnosis of thyroid eye disease correct?
Does the patient show any evidence of sight-threatening disease?
A thorough and detailed clinical history should be taken. Patients should be examined repeatedly and thoroughly with a special emphasis on tests of optic nerve function:
The patient’s best corrected visual acuity should be measured and recorded in each eye along with any refractive error.
The pupil responses should be carefully assessed, looking for the presence of a relative afferent pupil defect.
The patient’s color vision should be tested. Testing in the blue–yellow axis is far more sensitive and more likely to detect early color vision defects associated with CON. Red–green pseudoisochromatic charts (e.g., Ishihara color plates) are more readily available in clinics and remain very useful. Each eye should be tested separately using good illumination. The patient should wear his or her reading glasses to undertake the test. This assumes that the patient does not have color blindness. In such patients visual-evoked potentials (VEP) can be used. The pattern-reversal VEP is very sensitive at detecting early CON and may also be a useful means of following patients after treatment.
The patient should undergo automated perimetry. Characteristically, a central scotoma or an inferior altitudinal defect is seen in patients with CON. Other visual field defects include an enlarged blind spot, paracentral scotomata, nerve fiber bundle defects, or a generalized constriction.
Careful fundoscopy should be undertaken, looking for optic disc swelling or choroidal folds.
The patient’s proptosis should be measured using a Hertel exophthalmometer.
The patient’s palpebral apertures should be measured.
The patient’s levator function should be measured. The degree of lid lag on downgaze and the degree of lagophthalmos on passive eyelid closure should be recorded.
An orthoptic evaluation should be undertaken, recording the patient’s ocular motility restrictions, the field of binocular single vision, and a Hess chart. A preexisting strabismus will inevitably complicate this assessment. Pain on ocular motility should be documented. All inflammatory signs should be recorded. The corneas should be carefully examined for signs of exposure keratopathy.
The intraocular pressure should be measured in the primary position, downgaze, and upgaze.
Clinical photographs should be taken as a baseline assessment for later comparison.
Two additional aspects should be considered in the evaluation of patients with thyroid eye disease:
The activity of the disease.
The severity of the disease.
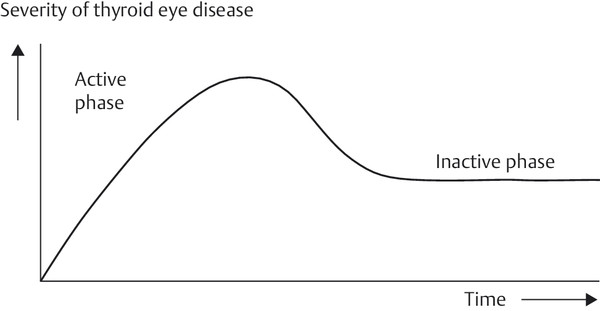
During the course of thyroid eye disease, the disease process passes through several phases. The initial phase involves worsening symptoms and signs with orbital inflammation, followed by a plateau phase during which the symptoms and signs become stable. A phase of gradual spontaneous improvement follows until eventually no further change occurs, although permanent abnormalities of both ocular function and cosmetic appearance may remain. These phases, however, vary greatly in duration from patient to patient. The typical course of thyroid eye disease in patients receiving no specific treatment, except that to control thyroid dysfunction, was first described by Rundle in 1957. He depicted this in a graph, which is known as Rundle’s curve (Fig. 20‑18).
The activity of the disease is determined clinically by the patient’s soft tissue symptoms and signs. It can also be determined by short Tau inversion recovery (STIR) sequence magnetic resonance imaging (MRI) that suppresses the normal bright signal from orbital fat on T1-weighted images.
The severity of thyroid eye disease describes the degree to which ocular function or the patient’s cosmetic appearance is affected. The severity is determined by assessing the effect of the disease on the following:
Optic nerve function.
Ocular motility.
The cornea.
The position of the eyelids.
The position of the globe.
The patient’s cosmetic appearance.
Determining the activity and severity of thyroid eye disease at each clinical assessment is fundamental to formulating a management plan, which is tailored to the individual needs of the patient.
A number of classifications of the ophthalmic changes in thyroid eye disease have been described in an attempt to quantify the orbitopathy. The classification by Werner was frequently used because of the easily remembered mnemonic NOSPECS. This acronym refers to No physical signs or symptoms, Only signs, Soft tissue involvement, Proptosis, Extraocular muscle involvement, Corneal involvement, and Sight loss. Although widely used, there are many difficulties in applying this and other classifications. The preferred classification is that of Mourits et al., who devised the clinical activity score (CAS) in 1989 (Box 20.1). This scoring system allows patients to be classified as either active or inactive, although some clinical features may reflect orbital congestion rather than inflammation. It indicates the position of the patient on Rundle’s curve. Although no scoring system is perfect, NOSPECS remains a useful reminder of the clinical features that should be assessed.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


