20 Endoscopic Latissimus Dorsi Flap Reconstruction
The introduction of minimally invasive techniques in aesthetic plastic surgery in the 1990s has proved to be an extremely useful addition; however, reconstructive surgery has been slower to incorporate these techniques. The harvesting of the latissimus dorsi muscle for pedicled and free flaps is one area in which minimally invasive approaches have been used with some frequency; this technique reduces scarring and potentially decreases donor site morbidity.
When compared directly with traditional harvesting techniques for microvascular reconstruction, the endoscopically assisted harvest of the latissimus dorsi muscle results in improved postoperative pain, better ipsilateral upper extremity activity, and significant improvement in patient scarring and patient satisfaction. 1
In 1993 Friedlander and Sundin 2 reported using the endoscope for harvesting the latissimus dorsi muscle in cadaver and porcine models. Clinical uses were later reported mainly for lower extremity defects. 3 , 4 John Bostwick 5 popularized the use of this technique to fill partial mastectomy defects.
Patient Selection
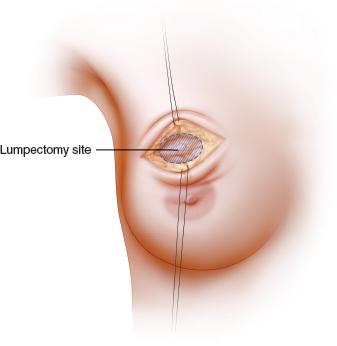
If a patient has small breasts or insufficient residual breast tissue for remodeling procedures or wishes to maintain her breast size and shape without altering the opposite breast, the endoscopically assisted technique is very useful. It is more commonly used for immediate reconstruction of partial mastectomy defects when volume only is required. An endoscopically harvested latissimus dorsi flap can be used for defects in almost any location; however, its use becomes more difficult for correction of medial quadrant defects. This illustration shows an upper pole lumpectomy defect with volume loss above the nipple, with no deficiency in skin coverage. If closed primarily, this defect could result in contour irregularities after radiotherapy.
The Decision-Making Process
After deciding that the latissimus dorsi flap is required for immediate volume replacement of the partial mastectomy defect, the most appropriate timing for the reconstruction must be established. It is often safer to confirm clear margins before proceeding with the flap reconstruction.
Because positive tumor margins on final pathologic evaluation could potentially compromise the reconstruction, it is imperative that this confirmation be obtained before the flap reconstruction.
Surgical Plan to Assess the Tissue Deficiency After the Quadrantectomy
Confirm negative margins (delayed-immediate reconstruction).
Harvest the latissimus dorsi muscle and subcutaneous tissue.
Minimally extend the axillary dissection incision and incise along the lateral portion of the latissimus dorsi muscle for access.
Infiltrate the wetting solution and pretunnel to reduce bleeding.
Undermine the skin below the subdermal plexus.
Elevate the flap and divide along the lateral edge of the latissimus dorsi muscle and inferiorly.
Separate the flap from the teres major muscle to the tip of the scapula and divide the medial aspect of the latissimus dorsi muscle.
Identify the pedicle.
Release the insertion and rotate and inset the flap.
Place drains and close the donor site.
Operating Room Setup And Patient Positioning
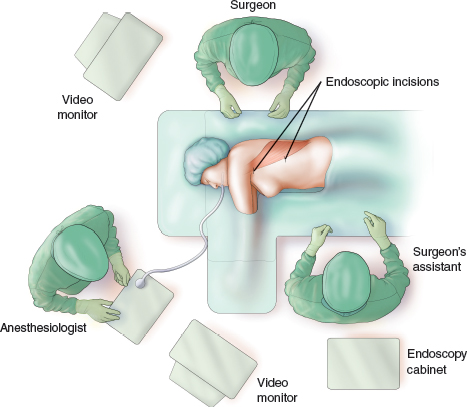
The operating room setup and patient positioning are the same for harvesting either a pedicled or a free latissimus dorsi muscle. As illustrated, the patient is placed in the preferred lateral position, with the ipsilateral arm prepared widely to allow repositioning during the pedicle dissection and tendon division. This position allows optimal exposure, visualization, and orientation for the surgeon and assistant. Occasionally, for smaller defects that require a relatively small portion of the flap, the patient can be placed in the supine position for segmental harvest of the anterior section of muscle.
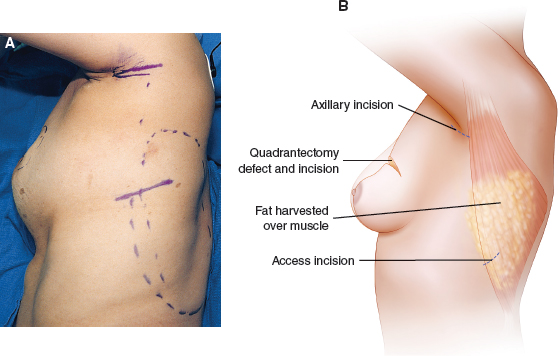
The patient is marked preoperatively in the standing position (A). The amount of volume required is anticipated by evaluating the films and the size of the defect and by communicating with the respective surgeon. The borders of the muscle are drawn out and the proposed incisions are marked. Axillary and lateral chest incisions are used for muscle access (B). Wetting solution is infiltrated in the subcutaneous tissue overlying the latissimus dorsi muscle. Occasionally, a single 5 to 7 cm access incision can be positioned about 5 cm caudal to the axillary fossa at the posterior axillary line, anterior to the lateral border of the latissimus dorsi muscle. This is often possible if the muscle length is less than about 20 cm. The entire flap can be harvested through this incision. The two-incision approach is preferred and allows smaller incisions to be used; it also allows accurate identification and protects the pedicle. A small axillary incision is often already there from the nodal dissection, and it can be used for the harvest.
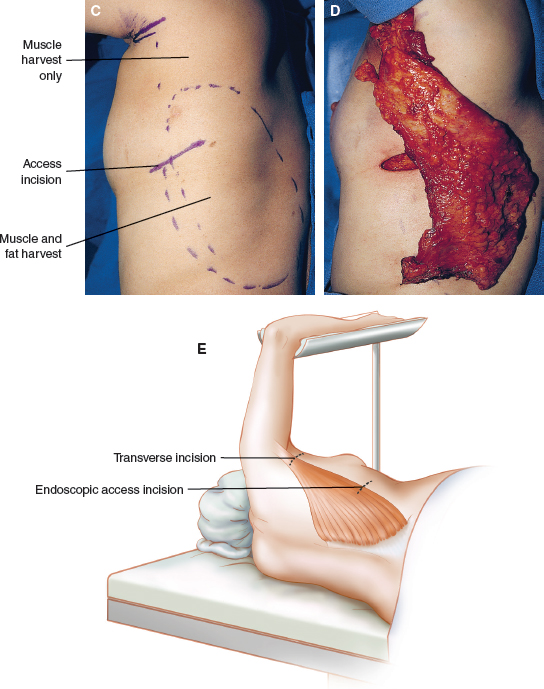
The latissimus dorsi muscle is harvested along with the overlying subcutaneous tissue, which is pretunneled over the entire extent of the muscle. The top of the axilla is dissected to minimize the bulk of the muscle itself and of the lateral breast tunnel (C and D). As on this patient, the flap is dissected in the subcutaneous plane, and the lateral margin of the latissimus dorsi muscle is identified. The latissimus dorsi muscle is elevated off the serratus anterior muscle. The thoracodorsal vessels are dissected under direct visualization through the axillary incision to ensure safety of the pedicle before its dissection off the chest wall. The dissection is initiated with direct visualization. The endoscope is inserted through the axillary incision, and the lateral margin of the latissimus dorsi muscle is dissected almost to the extent of the endoscopic incision inferiorly (E). The interval between the latissimus dorsi and teres major muscles is identified using the endoscope, and the dissection is extended down to the tip of the scapula. The endoscope is then positioned through the lateral incision, and the dissection proceeds to the interval between the serratus anterior and latissimus dorsi muscles, separating these structures and preserving the crossing branch on top of the serratus anterior muscle.
It is important to maintain the dissected optical cavity to allow visualization, often with the aid of a Deaver or an Emory endoscopic retractor with an endoscope, which is attached to a video monitor. Submuscular dissection can be performed bluntly; however, any perforating vessels off the chest wall should be clipped and transected. The extended Bovie electrocautery unit is used with a bent tip or specially designed endoscopic scissors with electrocautery. A third small incision is occasionally required along the upper medial border of the muscle if adequate visualization of the instrumentation is not possible because of the chest wall curvature. The dissection of the optical cavity should extend beyond the marked recipient defect to facilitate hemostasis after division of the distal muscle. The latissimus dorsi muscle is then divided inferiorly and medially using electrocautery and endoscopic assistance.
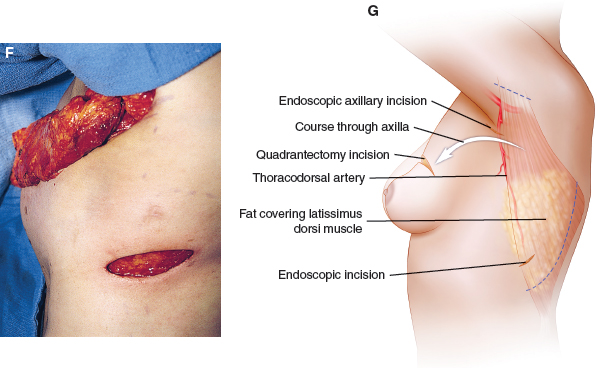
The latissimus dorsi is dissected completely on its vascular pedicle and passed through the subcutaneous tunnel into the axillary incision (F and G).
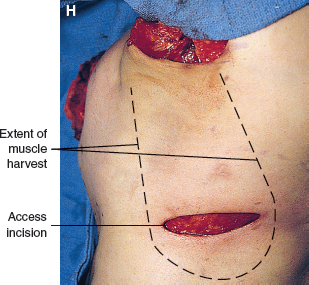
The humeral insertion of the latissimus dorsi muscle is divided to facilitate flap movement into the breast and to minimize any postoperative animation. Muscular denervation is typically not performed, because this causes additional atrophy. The flap is passed from the axillary incision into the partial mastectomy defect (H).
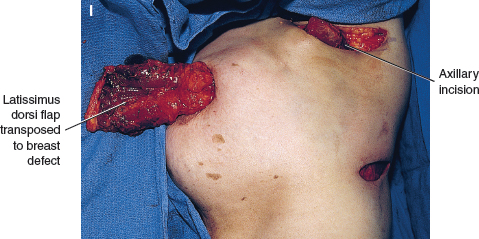
The latissimus dorsi muscle is brought out of the breast through the quadrantectomy incision (I).
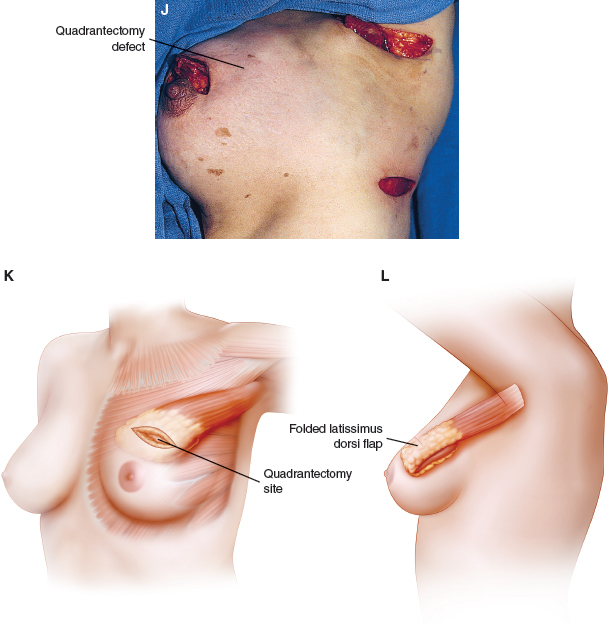
The muscle is folded on itself to add bulk, then is positioned to fill the defect and provide good contour for shape preservation and symmetry (J through L).
Patient Example
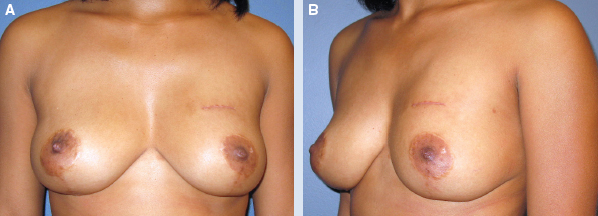

This 34-year-old woman previously had a breast reduction and presented to the surgical oncologist with left-sided breast cancer at the 12 o’clock position (A and B). The patient preferred to preserve her breasts and opted for a partial mastectomy. A moderate resection was performed; however, margins remained involved. The surgeon and patient discussed the possibilities of undergoing a mastectomy or attempting further reexcision. The patient still desired breast conservation, and she expressed concerns about further contour distortion with additional resection.
To allow a generous resection that would also ensure negative margins and preserve breast shape, the patient was referred for partial breast reconstruction. She presented with decent shape, although she had a scar in the upper pole (C and D). It was believed that an additional resection would further compromise her shape and result in a BCT deformity. To prevent this outcome, additional volume was required. There was no skin lost with the resection, and the deformity was not a complication from radiotherapy. Therefore skin was not required with the reconstruction, only volume. The patient was concerned about scars, and the decision was made to harvest a latissimus dorsi flap using an endoscope.
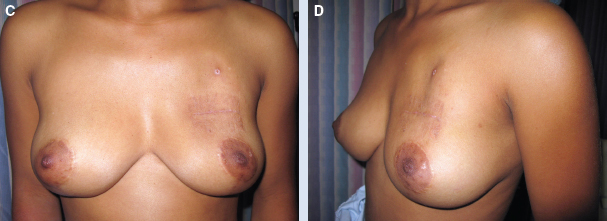
Because flap reconstructions can be compromised if the new margins are still positive, the reconstruction was deferred until her margin status was confirmed. A generous reexcision was performed that resulted in an upper pole contour deformity, despite being filled with seroma fluid (E and F). The patient’s margins were clear after reexcision, and she was taken back to the operating room for reconstruction of the partial mastectomy defect. In the decubitus position, an endoscope was used to harvest the latissimus dorsi muscle through two small access incisions. The humeral insertion was taken down, and the flap was transferred to the upper pole.
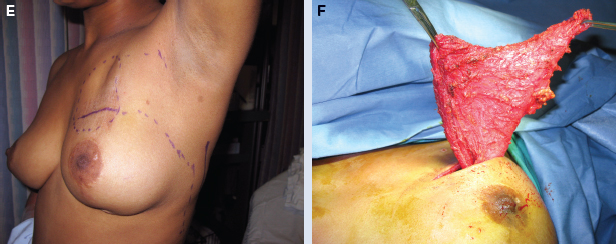
The donor incisions were then closed over drain suction, and she was prepped again in the supine position. The latissimus dorsi myofascial flap provides vascularized tissue with sufficient bulk, under no tension, before it is inset (G). The flap is then contoured and inset with precision to correct the volume and preserve the shape of the upper pole. The cavity is clipped for postoperative surveillance. The volume is typically overcorrected in anticipation of potential radiation fibrosis.
The patient is shown in all stages of her treatment: preoperatively after moderate resection (H and K), after reexcision (I and L), and 6 months after surgery (J and M). Her final outcome is good—the shape and symmetry of her breast have been preserved, and there is improvement in the contour of the upper pole.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


