19 Nerve Repair in the Hand
Abstract
Functional recovery after nerve injury in the hand requires special attention to primary repair and reconstructive principles in order to optimize outcomes. The surgeon must have various reconstructive tools available to address all possible scenarios, with the goal being to achieve a tension-free repair site. There are myriad commercial reconstructive options available to bridge nerve gaps and defects, but nerve autograft currently remains the gold standard for nerve reconstruction. Despite optimal surgical technique, nerve function seldom returns to its preinjury status, with perhaps exception to the pediatric population.
19.1 Description
Neglected nerve injuries in the hand frequently result in severe pain and disability. Nerve repair or reconstruction can improve functional recovery and outcome. Unfortunately, most patients fail to recover normal nerve function after trauma to a peripheral nerve. Consequently, the goal of nerve repair is to utilize the most appropriate technique to achieve a tension-free repair site and thereby optimize recovery.
Often, nerve injury in the hand does not occur in isolation. Other injured structures should be repaired concomitantly if possible. The inflammatory response to trauma and the immobilization necessary to allow healing of injured bones, tendons, arteries, and skin can negatively affect the final outcome of nerve recovery. 1
19.2 Key Principles
Many independent factors affect recovery after nerve injury. Important factors that cannot be controlled for at the time of surgery include patient age, mechanism of injury, and delay in diagnosis. Younger patients have improved recovery of motor and sensory function after peripheral nerve repair. 1 , 2 Also, recovery of sensory nerve function after sharp laceration is better than nerves injured by crush mechanisms. 1
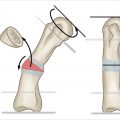
The timing of nerve repair is also an important factor. Primary repair or direct coaptation can usually be performed within a few days of the injury, and the nerve’s landmark vasculature is more easily identifiable to guide alignment of the neurorrhaphy site. After a period of time, the nerve’s elasticity decreases, which results in nerve gaps with attempts at primary repair. Nerve elasticity decreases as Wallerian degeneration occurs in the injured nerve. 3 Nerve defects can also result when the zone of injury is larger, such as in a saw injury (► Fig. 19.1).
The goal of any nerve repair or reconstruction is a tensionfree repair site. Nerve healing and axonal regeneration requires adequate blood flow, and excessive tension across the repair site decreases blood flow. An animal study by Clark et al 4 evaluated nerve blood flow in an animal model. These researchers demonstrated that a 15% increase in tension across the repair site decreased the blood flow by 80%. Also, when a 16 to 17% increase in tension was applied to the repair site, it resulted in suture pullout and failure of the repair. These findings illustrate that lack of blood flow is likely the mechanism for nerve repair failure prior to disruption of the repair site. 4 If a tension-free repair is not obtainable, the surgeon should consider any number of reconstructive techniques to bridge the gap and provide a tension-free repair.
19.3 Indications
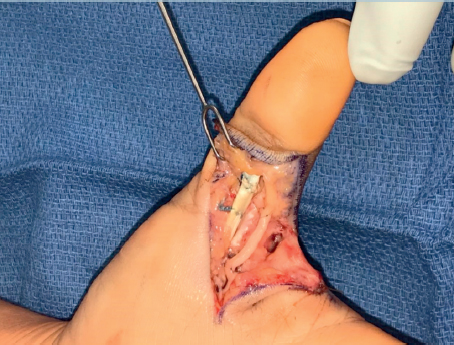
Any nerve injury in the hand should be considered for repair or reconstruction. Painful neuromas may result from a neglected sensory nerve injury, and functional loss occurs from injuries to the motor branches of the median and ulnar nerves. Frequently, procedures such as fracture fixation, tendon and blood vessel repair, and soft tissue reconstruction can be performed at the same setting as nerve repair (► Fig. 19.2).
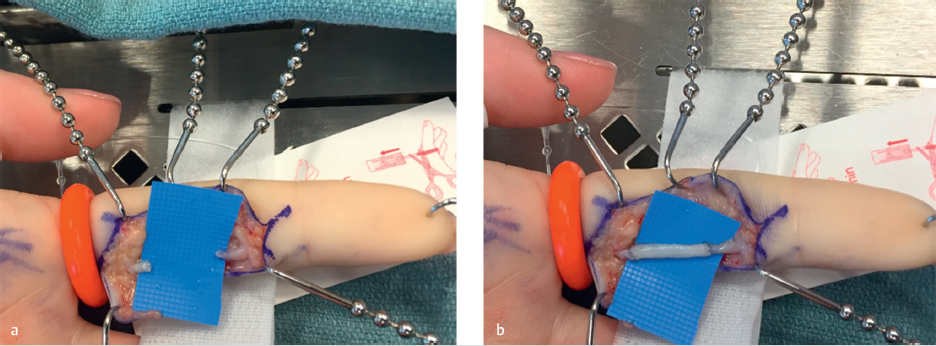
If primary nerve repair or direct coaptation is not possible, then the surgeon needs to have a backup plan utilizing the reconstructive ladder of nerve conduits, autograft, and processed allograft. Nerve conduits are indicated for sensory nerve reconstruction with gaps up to 3 cm and function to give the sprouting axons a directional channel for regeneration. 5 Commercially available artificial conduits are typically composed of collagen, caprolactone, or polyglycolic acid (PGA). In their study of 22 digital nerves reconstructed with collagen conduits, Taras et al 5 demonstrated a moving and static 2-point discrimination of 5.0 and 5.2 mm, respectively, at a mean follow up of 20 months after surgery. 5 Processed nerve allografts used to span digital nerve gaps of less than 3 cm resulted in an average static 2-point discrimination of 7.1 mm in 21 digital nerves. 6 Commercially available processed nerve allografts were studied in the RANGER study, and are indicated for nerve gaps between 5 and 50 mm in digital sensory nerves and motor or mixed nerves. These researchers found meaningful recovery in 89% of digital sensory nerves, 75% of median nerves, and 67% of ulnar nerves. 7 Nerve gaps greater than 5 cm are best reconstructed with vascularized nerve graft techniques.
Nerve autograft, which is still considered the gold standard for nerve reconstructions, can be harvested from one of several donor sites depending on the diameter of the injured nerve. The sural nerve in the lateral leg can be used to graft defects between the wrist and the common digital nerves. Convenient nerve donors in the ipsilateral extremity include the terminal branch of the posterior interosseous nerve at the wrist’s 4th dorsal compartment, and the lateral and medial antebrachial cutaneous nerves in the forearm. These donor nerves can be used to reconstruct digital nerve defects. 3
19.4 Contraindications
The medical stability of the patient takes priority over the nerve injury. The patient must be medically stable to undergo the planned anesthetic, and the wound must not exhibit any signs of infection.
19.5 Special Considerations
Long-term studies of patients following nerve repair have demonstrated that the younger the patient, the better the outcome in terms of nerve recovery. 2 While advanced patient age is not a contraindication to nerve repair surgery, age must be considered in the setting of severe proximal injuries that require reconstruction. The surgeon must also weigh the risks and benefits of surgery in the elderly population against the risk of painful neuroma development if surgical repair is not performed.
Primary repair of motor nerve branches of the median and ulnar nerves in the hand require special attention to the alignment of nerve fascicles. At the level of the wrist, grouped fascicular repairs of the sensory and motor components can be performed, since these components can often be identified and separately repaired or reconstructed.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


