18 The Role of Local Flaps as Volume Replacement in Oncoplastic Reconstruction
Despite the recognition that most breast-conserving surgery (BCS) defects can be treated with primary closure, the aesthetic outcome may be unpredictable and occasionally can be complex to reconstruct. 1 , 2 Recently increasing attention has been focused on reconstructive techniques. 1 – 13 Basically, two different groups of oncoplastic procedures exist, and the choice of which technique to perform depends on the volume of the excised breast tissue related to the total breast volume and degree of ptosis. One group of techniques is commonly defined as volume displacement procedures, which combines resection with a variety of different breast-reshaping and breast-reduction procedures; the other group is defined as the volume replacement procedure in which the volume of excised breast tissue is replaced with autologous tissue. In fact, these techniques can retain the volume and shape of the breast and avoid contralateral breast surgery. However, these techniques can be more complex and require a donor site and increased recovery time following flap harvesting.
Local flaps are relatively simple techniques that reconstruct with tissue of similar color and feel and can maintain the volume/shape of the breast, avoiding contralateral surgery.
Among the main technical options, local flaps, 1 , 3 , 6 , 8 the latissimus dorsi myocutaneous flap, 1 , 6 , 7 and reduction mammaplasty 1 – 4 , 9 – 13 are the most commonly employed techniques with more favorable outcomes. Regardless of the fact that there is no consensus concerning the best approach, the decisive criteria is determined by the surgeon’s experience and the size of the defect in relation to the size of the remaining breast. 1 , 3 , 7 – 10 The main advantages of the technique utilized should include reproducibility, low interference with the oncologic treatment and long-term results. Probably, all these goals are not achieved by any single procedure and each technique has advantages and limitations. 9
In terms of aesthetic results and surgical morbidity, local flaps have some positive aspects. The skin texture and color are comparable, the technique is simpler, and the operative process is less aggressive. 8 All these factors are important, because some patients will undergo adjuvant chemotherapy and radiotherapy. Local flaps have been described previously. 3 , 8 , 14 – 17 Basically, the major part of the techniques have employed a rotation or transposition flap of skin and subaxillary fat for the breast defect. 8
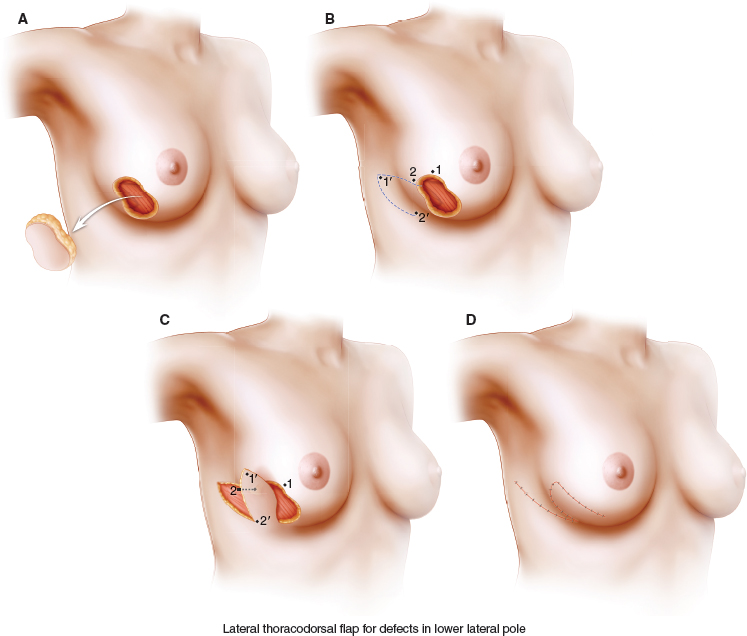
Initially described by Holmstrom and Lossing in 1986, 18 the lateral thoracodorsal flap is a commonly performed procedure for delayed radical surgery reconstruction. The flap can be planned as a wedge-shaped transposition design located in the lateral aspect of the thorax. The axis is located in the lateral extensions of the submammary fold. Its major clinical application is in patients who refuse higher morbidity procedures or are not good candidates for more extensive reconstruction, particularly with myocutaneous flaps. 8 , 18
In spite of the simplicity of the technique, important technical steps must be considered beforehand. Operative planning should include tumor location and the extent of glandular tissue resected, essentially addressing individual reconstructive requirements. Thus enabling each patient to receive an individual “customized” reconstruction. The success of the procedure depends on patient selection, coordinated planning with the oncologic surgeon, and careful intraoperative management. In addition, an in-depth dialog concerning alternatives for BCS reconstruction should be undertaken with the multidisciplinary scenario, including the risks and positive aspects of the local flap reconstruction.
Delayed-Immediate Local Flap Reconstruction
Volume replacement procedures and the use of local flaps can be indicated for immediate, delayed, and delayed-immediate reconstructions. The advantages of each approach are described in Chapter 13.
Indications for use of Local Flaps with Oncoplastic Techniques
Partial breast defects represent an anatomic variety that ranges from small defects to large defects that involve skin, nipple-areola complex (NAC), and a significant amount of glandular tissue. Each defect has its own special reconstructive necessities and varying expectations for aesthetic outcome.
Although a number of reconstructive procedures are available, the surgeon and patient need to consider a number of factors when selecting the most appropriate approach. Adequate selection depends on a range of features, including breast size/ptosis, tumor location, timing of surgery, morbidity, and patient expectation. Volume replacement techniques can maintain the volume and shape of the breast, avoiding contralateral surgery to attain symmetry. 7 , 19 However, these techniques can be more complex procedures associated with donor site and flap morbidity. 6 , 7
Volume replacement procedures is defined when the resection defect is reconstructed by replacing the volume of tissue removed with a similar volume of autologous tissue from an extramammary region. 19 This restores the breast volume and avoids the need for contralateral surgery to achieve symmetry. As opposed to breast volume displacement techniques the concept of breast volume replacement using local flaps has some advantages. The main indication for local flaps is the absence of some remaining breast tissue. 7 , 8 This is true primarily in patients with small-volume breasts with or without ptosis. It includes patients with moderate lateral defects where there is not enough breast tissue to perform the reconstruction by local glandular flaps or reduction mammaplasty techniques. 8
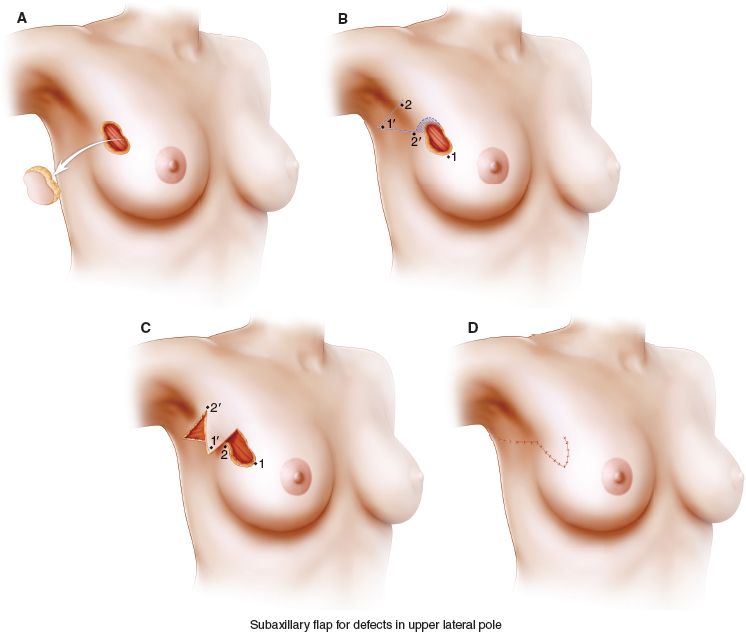
Recently, different techniques of local flaps have been proposed for reconstruction after BCS. 1 , 3 , 8 , 14 – 17 Fundamentally, these procedures all rely on rhomboid flaps, lateral thoracodorsal flaps, and subaxillary flaps. The majority of techniques involves the use of excess skin and subcutaneous tissue in the lateral thoracic region. 8 When a large local flap is necessary a modification of the lateral thoracodorsal flap can be planned to harvest a flap carrying a large amount of skin and fat tissue. For this purpose a convex flap design, which provides a large amount of skin and makes the base narrower to avoid wound tension closure, is used. Since the axis is located in the lateral/dorsal extensions of the submammary fold, its major clinical application is in patients who refuse major morbidity procedures or are not good candidates for more extensive autologous tissue reconstruction. 8
In spite of these positive aspects, local flaps present some limitations. Preoperative patient evaluation is crucial to determine the amount of tissue available and to allow optimal positioning of the tumor incisions to avoid an ischemic flap. Moreover, for the tumors located in the lower outer quadrants, a wide undermining below the inframammary sulcus during tumor resection may jeopardize flap vascularization and favor complications. 8 For this reason, a coordinated planning with the oncologic surgeon is imperative with discussion of the surgical approach. Since some local flaps are not axial flaps, vascularization to the most distant parts is difficult to predict. 1 , 8 , 20 This situation can predispose to partial necrosis (skin and fat) and an undesirable result.
Typically, lateral thoracodorsal flap reconstruction is most appropriate for women with small- or medium-sized breasts with large defects, who are not good candidates for volume displacement procedures. 8 Other volume replacement techniques such as the subaxillary flap 14 , 15 and the rhomboid flap are better indicated when reconstructing less extensive BCS defects.
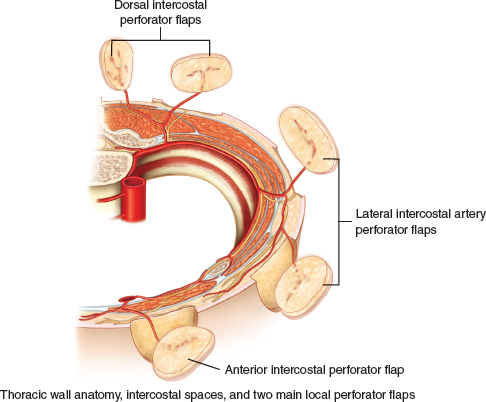
Although presently BCS defect repair is the main objective, minimizing donor-site morbidity has now become an important point in surgical planning. For this purpose a number of local perforator flap techniques are available and the choice of procedure depends not only on an aesthetic outcome of the reconstructed defect but also on the reconstructive and functional requirements. Usually, the lateral thoracic area contributed to potential alternatives for perforator flaps. The use of the intercostal perforator vessels to supply a skin-muscle flap has been described and some authors divided the intercostal region into four anatomical segments: vertebral, costal groove, intermuscular, and rectus. 21 , 22 , 23 Thus based on the anatomy of the main perforator vessels, different perforator flaps can be harvested to repair partial breast defects without significant technical complications and with oncologic results comparable to other oncoplastic procedures. It has been our impression that the application of perforator concept to local flaps has greatly expanded the range of alternatives available. Therefore the present technique broadens the range of local flap applications and decreases donor-site morbidity. Variations of the local perforator flaps will become potential alternatives as reconstructive surgeons become more familiar with its anatomy, planning and clinical applications.
Operative Technique
The Rhomboid Flap
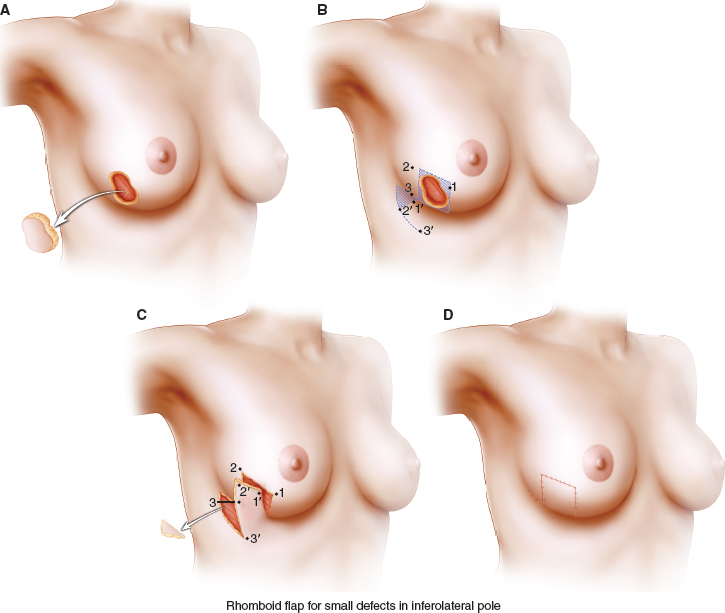
Classically, a rhombus is defined as an oblique-angled parallelogram, whereas a rhomboid differs in that it has uneven adjacent sides. The expression rhomboid is commonly used in facial reconstruction to represent either rhombus-like defects or to illustrate one of the popular transposition flaps used to repair rhombus-shaped defects. Rhomboid flaps are helpful when the size or shape of a breast skin defect does not permit direct closure using a fusiform incision. In some BCS defects, attempting to close a wide lumpectomy defect primarily requires an ellipse with either long limbs or blunt angles. Lengthy limbs create long scars and remove healthy tissue unnecessarily, whereas blunt ends often create an unpleasant standing-cone or dog-ear appearance. Additionally, the lack of skin and breast tissue and the deviation or distortion of the NAC can be observed.
Surgical Planning and Technique
Considerations when designing any rhomboid flap include the diameter of the breast tissue/skin defect, the amount of normal skin that needs to be redundant, the scar orientation with respect to relaxed skin tension lines, the arc of skin rotation, and the vector of maximal tension after closure. When designing a flap, if possible match the skin color and thickness and respect boundaries of breast aesthetic units. 24 Rhomboid flaps have been used in reconstruction of the lateral and inferior breast pole defects (see Fig.18-1, A). However, the aesthetic and mechanical properties of these flaps and especially the characteristics of the breast shape, make them particularly helpful for reconstruction of small BCS defects in the lateral quadrants. The flap and adjacent tissue are undermined in the subdermal plane after creating the rhombus defect (see Fig. 18-1, B and C). Rhomboid flaps are full-thickness local flaps with a random blood supply. Rather than depend on an axial blood vessel for nourishment, rhomboid flaps rely upon the dermal-subdermal plexus of blood vessels. If a large amount of tissue is necessary to fill the defect, the undermining can incorporate the surrounding breast tissue and fat. Lines of maximal extensibility lie perpendicular to skin creases. Tension is greatest at the closure point of the donor defect. The size and degree of undermining do not change the relative tensions of closure. It is important to place the line of maximum flap tension (the line of closure of the donor area) in a line of maximum extensibility of the breast. Primary tension of the closure must never displace a neighboring structure and the prominent landmarks, especially the NAC and the inframammary fold.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


