There are scenarios where the length of the digit cannot be preserved secondary to either significant trauma, or necrosis due to distal thrombosis of the digital arteries. Terminalization is warranted in these cases to provide a well-padded pain-free stump for the patient.
A fish-mouth incision is designed and the bone is cut back with rongeurs or an oscillating saw to allow for a tensionless closure. Important steps include burying and cauterizing the nerve stumps to prevent neuroma and avoiding the temptation of stitching the flexor and extensor tendons together over the bony stump (Fig. 18‑1, Fig. 18‑2, Fig. 18‑3, Fig. 18‑4, Fig. 18‑5, Fig. 18‑6, Fig. 18‑7, Fig. 18‑8, Fig. 18‑9).
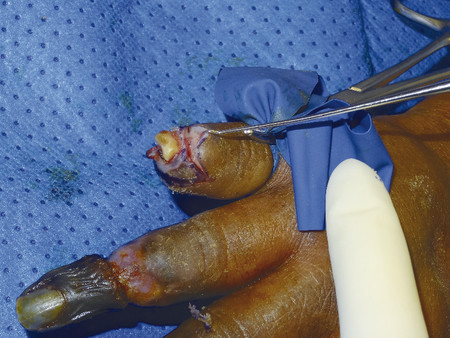
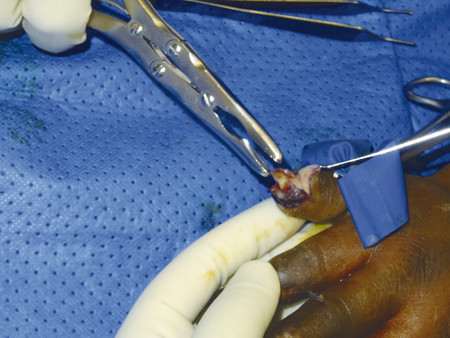
Fig. 18.1 Patient who developed necrotic fingertips after multiple emboli from the subclavian artery.Fig. 18.2 Necrotic segment is removed with a knife demonstrating exposed bone. A digital tourniquet is applied.Fig. 18.3 Fish-mouth incision is marked to allow closure of the stump after removal of exposed bone.Fig. 18.4 Flaps are raised in a plane just above the bone.Fig. 18.5 A rongeur is used to remove the bone. If the bone is hard, an electric saw can also be used.Fig. 18.6 A rasp is used to soften out sharp edges.Fig. 18.7 The digital nerve is identified and diathermied using bipolar then cut under tension so that it is buried. The digital arteries are cauterized.Fig. 18.8 4.0 Vicryl Rapide is used to close the stump, a padded well-protected stump is the result.Fig. 18.9 Final result.
Only gold members can continue reading. Log In or Register to continue