6 Hand Infections
6.1 Flexor Sheath Infection
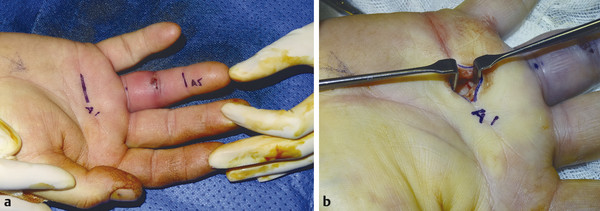
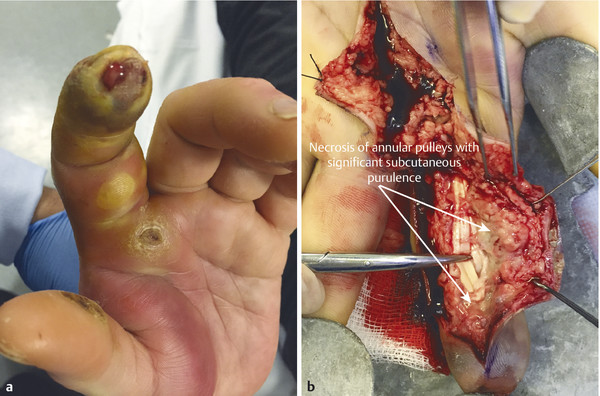
Flexor sheath infections are heralded by Kanavel’s signs: fusiform swelling, flexed posture to digit, pain over flexor sheath, and pain on passive extension (Fig. 6‑1). These infections should be treated with emergent washout to avoid chronic hand dysfunction and in severe cases amputation.

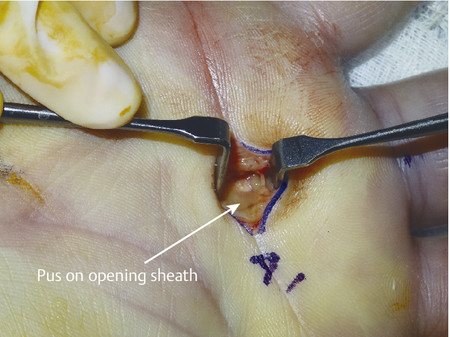
Early presentations without subcutaneous purulence can be washed with a closed technique and can be given intravenous antibiotics. Later presentations with subcutaneous purulence may need to be managed with an open approach using broad midlateral flaps to prevent flap necrosis.
6.2 Flexor Sheath Washout
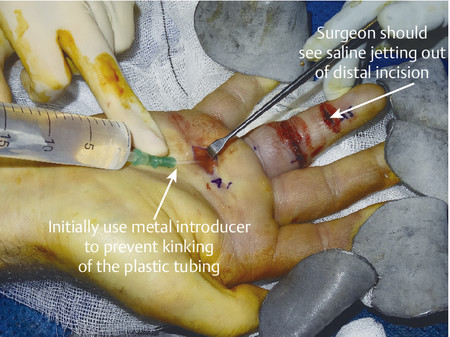
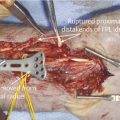
Once the flexor sheath is opened proximally, a green cannula with the metallic introducer is placed underneath the A1 pulley. The introducer maintains rigidity and prevents kinking of the plastic sheath. Sometimes due to swelling it is necessary to vent the A1 pulley to gain access. Distal access is made through the A5 pulley. If the surgeon remains midline, neurovascular structures will remain safe (Fig. 6‑2, Fig. 6‑3, Fig. 6‑4, Fig. 6‑5).

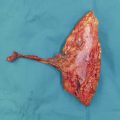
It is also important to lift the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) with a tendon hook to break up loculations and adhesions particularly if the patient is returning to theater for a second debridement (Fig. 6‑6).

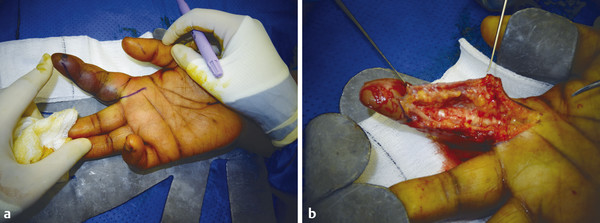
In cases where there is subcutaneous purulence or a closed technique has failed to improve the infection, an open approach is advised (Fig. 6‑7, Fig. 6‑8). Flaps should be kept broad to prevent tip necrosis and tendon exposure. A midlateral incision has a key advantage over a Bruner-type incision as the flap can cover the flexor tendons when the wounds are left open. Bruner flaps need to be at least tacked together to prevent retraction and tendon exposure.
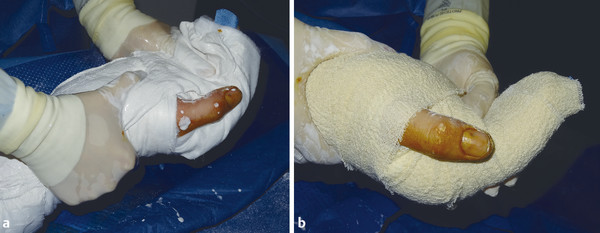
Wounds should be left open and dressed with Betadine-soaked gauze over Jelonet and a plaster of Paris in the position of safe immobilization (Fig. 6‑9, Fig. 6‑10). The injured hand should be placed in a high-arm sling to reduce edema.

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


