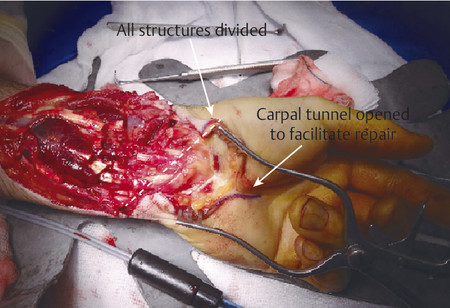
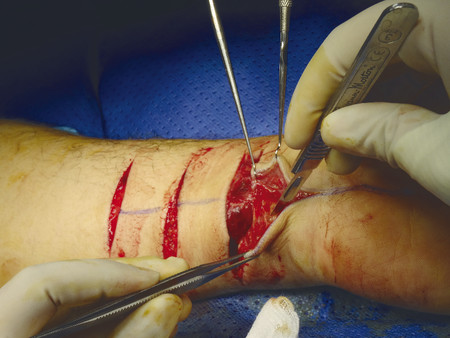
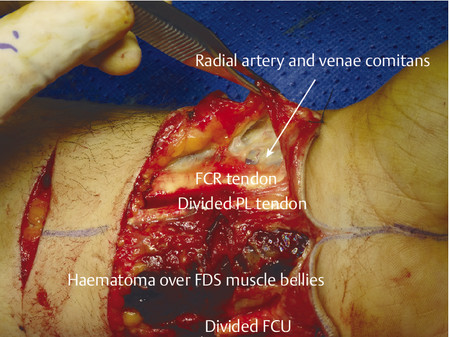
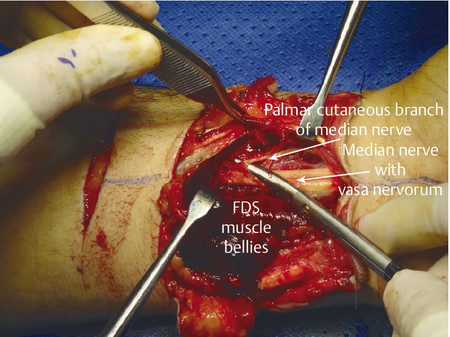
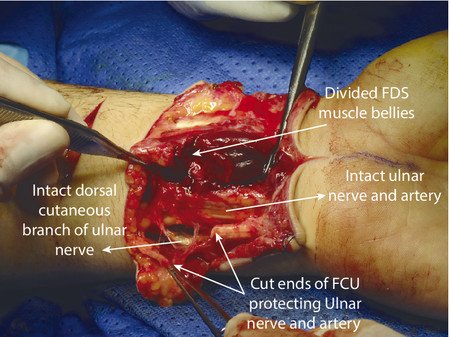
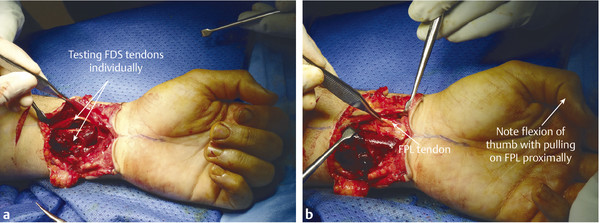
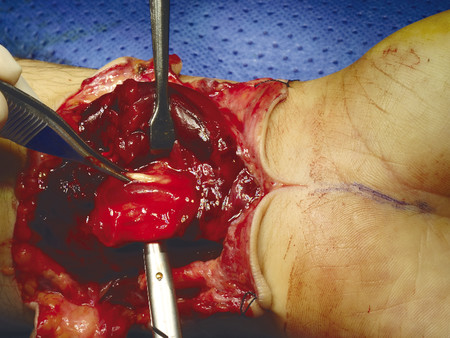
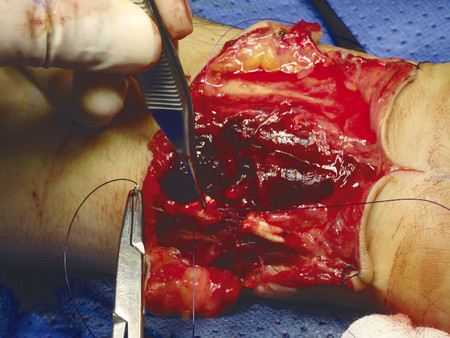
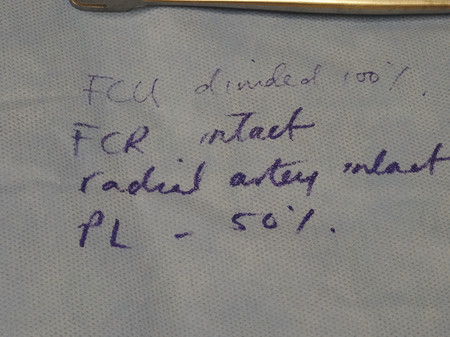
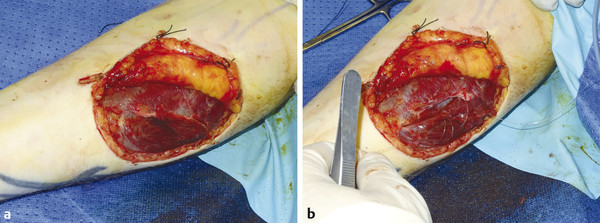
Fig. 13.1 Glass laceration to distal forearm with division of all structures including radial and ulnar arteries, the carpal tunnel has been opened to facilitate repair.Fig. 13.2 Broad flaps should be designed and flaps should be taken with fascia to minimize flap necrosis. The carpal tunnel may need to be opened to facilitate repair and should be marked.Fig. 13.3 Flaps being raised with fascia.Fig. 13.4 Dissection should be systematic and should start with the radial or ulnar side of the wrist with a systematic assessment identifying damaged structures. Here you can see the radial artery and flexor carpi radialis (FCR) are intact.Fig. 13.5 The median nerve is identified under the divided palmaris longus and its palmar cutaneous branch is also identified.Fig. 13.6 The figure shows the divided FDS muscle bellies and the FCU. The ulnar nerve and artery are not divided and were protected by the FCU tendon. The figure also shows the dorsal sensory branch of ulnar nerve.Fig. 13.7 (a) The FDS ring and the little finger are divided. The tendons are lifted to check each one individually. The FDS tendons to the ring and middle fingers are superficial to the index and small fingers. (b) The flexor pollicis longus (FPL) is the most radial structure in wrist and found to be intact if thumb flexion is present.Fig. 13.8 FDP tendons lie side by side and are brought up and found to be intact.Fig. 13.9 Repair of the FCU is with a four-strand modified Kessler 3.0 Prolene; note flexion of the wrist will help accommodate the repair. If the FCU has retracted back, a back wall 5.0 epitendinous stitch will help draw the tendon ends together making the core stitch easier.Fig. 13.10 Documentation of divided structures; important for the primary surgeon to keep track to prevent structures being missed.Fig. 13.11 Another case demonstrating completed median nerve repair with microscope using 8.0 Ethilon. The repair is epineural and the vasa nervorum have been used to align the nerve.Fig. 13.12 (a,b) Many surgeons use Vicryl to repair muscle bellies. However, using Monocryl has certain advantages; as it is monofilament, it glides easily and multiple continuous loops, as in the figures, bring the muscles together without difficulty.Fig. 13.13 Dorsal blocking splint to protect nerve and tendon repairs. Ensure the splint is securely taped on, so that it can last until it is changed for a thermoplastic splint.
Glass injuries are often more extensive than you think. One must perform a detailed preoperative examination so that you can identify which structures are likely to be damaged and which ones you must identify. One should start the dissection outside the zone of trauma to help identify normal anatomy, and then follow normal structures into the zone of trauma. This avoids ineffective dissection around the wound.
Only gold members can continue reading. Log In or Register to continue