18 Soft Tissue Fillers for Facial Augmentation
Key Concepts
Soft tissue facial fillers have developed into one of the most popular and widely used methods for facial rejuvenation.
Cross-linked hyaluronic acid (HA) products are among the most studied and versatile products and are used more than all other fillers combined.
The most common injection-site reactions are edema, erythema, tenderness, ecchymosis, and itching.
Treatment of impending skin necrosis consists of warm compresses, oral steroids, nitroglycerin topical paste for vasodilation, topical antibiotic ointment, hyaluronidase if HA was injected, hyperbaric oxygen, and/or deep subcutaneous heparin injection.
Introduction
The last decade has seen a tremendous increase in minimally invasive cosmetic procedures, most notably injectable synthetic soft tissue facial fillers. A better understanding of facial aging as a result of soft tissue atrophy has fueled this dramatic rise. These office-based procedures are fairly straightforward to perform, have minimal downtime for the patient, and, when combined with neurotoxins and laser skin treatments, can result in impressive rejuvenative outcomes. Today there are a wide variety of short-duration, long-duration, and permanent fillers available for use in the United States. This chapter reviews many of these products, with special emphasis on techniques to optimize the result while limiting complications.
Background: Basic Science of Procedure
Soft tissue volume restoration has received a greater amount of emphasis in the treatment of the aging face during the past 15 years. The idea of vertical facial descent with loss of elasticity being the main cause of facial aging has been supplanted by the idea that volume depletion occurs at multiple tissue levels, including skeletal and subcutaneous tissue.1–3 Facial beauty in a youthful face consists of fullness, softness, symmetry, and proper proportions. There is a smooth distribution and transition of skeletal and subcutaneous soft tissue between adjacent aesthetic zones of the face, with a resultant balance between volume and shape. Aging of the face involves tissue involution, with flattening and hollowing of facial features. Some of the earliest accounts of soft tissue augmentation utilized autologous fat over a century ago.4 Other permanent products, such as paraffin, were used at the end of the 19th century but were discontinued due to severe granulomatous reactions. Silicone has been injected for well over 50 years but was banned by the U.S. Food and Drug Administration due to concerns about its safety.5 Silicone is available today in 1,000 centistoke formulation for opthalmologic use and is utilized as an off-label cosmetic filler.6
The first widely used injectable fillers to be used in the United States were the bovine collagen products. They were introduced in the late 1970s and consisted of Zyderm and cross-linked Zyplast (Allergan, Irvine, CA) for the treatment of moderate fine lines and rhytids. The results were effective but short lived and resulted in about a 5% incidence of severe allergic reaction.7,8 Therefore, skin testing was required, which delayed patient treatments. The limitations of collagen products led to the development of longerlasting, nonallergenic, and more versatile fillers. Today, the emphasis in facial volume enhancement has been transformed from simple wrinkles and filling of folds to regional and panfacial augmentation.
Patient Selection
The ideal patient for injectable fillers has relatively good skin elasticity and minimal skin laxity. Patients with thin skin and limited soft tissue have an increased risk of visible irregularity of the injected product. Patients with chronic disease, especially autoimmune disorders, and pregnant or lactating females are not appropriate candidates for treatment.
Discussion of patient expectations, including correction and longevity, is critical in obtaining satisfactory results, and an explanation of the various fillers with benefits and limitations must be provided prior to the treatment. A thorough comprehension by both the clinician and the patient of the potential reactions and complications is necessary. Preinjection standardized photographs are imperative because results with fillers can be less noticeable than with surgical intervention.
Technical Aspects of Procedure
Ideal filler substances have FDA approval and are nonallergenic, noncarcinogenic, nonmigratory, easy to store, cost-effective, reproducible, durable, and malleable enough to provide a “natural” look and feel. The injection procedure should be relatively simple to perform, with minimal discomfort and with few adverse sequelae. Each product has its unique characteristics and is used differently in each patient. It should be noted that, although many surgeons use some of these techniques and products in the manner described, there may be off-label uses of the fillers.
Products can be categorized by the duration of the effect. Hyaluronic acids (HAs) are temporary fillers that have a lasting effect of ~ 6 months. Intermediate or semipermanent fillers have durations of up to 18 months and are composed of calcium hydroxylapatite (CaHA, Radiesse, Merz Aesthetics, San Mateo, CA) and poly-L-lactic acid (PLLA, Sculptra, Sanofi-Aventis U.S., Bridgewater, NJ). Permanent filler products available consist of Silikon 1000 (Alcon, Fort Worth, TX, off-label use) and collagen with polymethyl methacrylate (PMMA, Artefill, Suneva Medical, San Diego, CA). Products may be safely combined in the same patient during the same treatment session.
Techniques with previous fillers for simply filling lines on the face have been replaced with structural augmentation of deeper tissue levels with larger volumes of products. Evaluation of the face as a whole allows volume enhancement to be more comprehensive and to give a lifting effect to the face rather than treating only rhytids. A list of the facial regions with the author′s preferred products is provided in Table 18.1 . Product selection may vary with such factors as patient age, skin elasticity, and soft tissue thickness.
Patients undergoing soft tissue facial filler injections should be instructed to refrain from taking blood thinners, such as aspirin (as long as it is not medically necessary), nonsteroidal anti-inflammatory drugs, many vitamin supplements (vitamin E, fish oils, ginger, Ginkgo biloba, ginseng, garlic), and alcohol, ideally for 2 weeks prior to the injection. The procedure is performed using strict aseptic technique (alcohol or chlorhexidine), making sure the skin is cleansed of all dirt and makeup. A compounded topical anesthetic cream (20% benzocaine, 6% lidocaine, 4% tetracaine, Pharmacy Creations, Randolph, NJ) is applied to the treatment area for at least 10 minutes, with local injectable anesthetics sometimes being used, especially in the perioral region (dental block). The incorporation of lidocaine within most of the current products has greatly reduced discomfort associated with the injection. Ice is applied to the face prior to, during, and after the injection.
Hyaluronic Acid (Restylane, Perlane, Juvederm)
Cross-linked HA products are among the most studied and versatile products, have become the standard in the United States, and are used more than all other fillers combined. HA is naturally occurring in the skin but it has a very short half-life due to its sensitivity to hyaluronidases and is therefore cross-linked in the manufacturing process to prevent degradation. HA is obtained through the fermentation of Streptococcus equi. HA fillers are biocompatible, stable in vivo, safe, effective, and well tolerated.9
The most popular HA products used in the United States today are Restylane, Perlane (Medicis Pharmaceutical, Scottsdale, AZ, Q-Med AB, Uppsala, Sweden), Juvederm Ultra XC, and Juvederm Ultra Plus XC (Allergan, Irvine, CA). They are all FDA approved for implantation into the mid-to-deep dermis for the correction of moderate to severe facial wrinkles and folds, such as nasolabial folds. The concentration of HA is 20 mg/mL for Restylane and Perlane and 24 mg/mL for Juvederm Ultra XC and Ultra Plus XC. Ideally, Juvederm Ultra XC and Restylane can be injected with either a 30-gauge half-inch or a 29-gauge half-inch needle. Juvederm Ultra Plus XC and Perlane are most commonly injected with a 27-gauge half-inch needle. All the foregoing products are cross-linked in a phosphate buffer with 0.3% lidocaine, which significantly reduces pain at the injection site.
Juvederm products are monophasic, where 100% of the HA molecule is cross-linked, and Restylane (smaller gel particle size) and Perlane (larger gel particle size) are biphasic products, where they contain both cross-linked and un-cross-linked HA. Juvederm has a higher degree of cross-linking between HA molecules (6 to 8%) and is supplied in 0.8 mL syringes versus 2% for Restylane, which is supplied in 1 mL syringes. The higher percentage of cross-linking between HA molecules increases the viscosity of the material (reduces the ability to flow) and theoretically lasts longer.
Injection techniques vary with the injector and may include serial puncture, linear threading, crosshatching, or deep depot injections for regional augmentation. The filling effect of these products is a result of displacement of tissue and the hydrophilic properties, which attract water to the injection site. The author′s preference is using Juvederm Ultra Plus XC and Perlane for deeper dermal or subcutaneous injections, such as the nasolabial folds, for supraperiosteal injections in areas such as the prejowl sulcus, and for volume restoration to the upper cheeks. Juvederm Ultra XC is a preferred product for lip augmentation because it results in a smoother and broader augmentation as compared with Restylane.
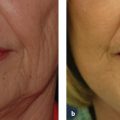
Restylane is the product of choice for tear-trough correction because it has a less characteristic hydrophilic effect and produces less edema Video 18.1. The technique involves using a minimal amount of local anesthetic to block the infraorbital nerve and to inject the filler using a 0.7 mm microcannula (Tulip, San Diego, CA). Other, newer, disposable, blunt-tipped cannulas are also available in 25 and 27 gauge by 1-, 1.5-, and 2-inch length (TSK Laboratory, Tochigi-Ken, Japan). The advantage of blunt-tip cannulas over standard needles is the ability to inject large volumes with less trauma, edema, and bruising and with a reduced risk of injecting into arteries or vessels. A sharp needle is used to make the entry site in the mid cheek, and the cannula is used to deposit small aliquots of material in the tear-trough deformity. It is imperative to inject at the level of the supraperiosteal tissue plane, to massage the material to the desired position, and not to overcorrect. Often, Restylane is diluted with 0.2 to 0.3 mL of 1% lidocaine, utilizing a transfer syringe, to reduce the hydrophilic effect of the material in this area of extremely thin skin. The hydrophilic effect of Juvederm is more pronounced and may result in visible accumulation of product in the tear trough or in the Tyndall effect. Therefore, if Juvederm is to be used in the tear trough, undercorrection is advised. HAs also have the added safety advantage of allowing one to correct excess fullness or superficial placement simply by injecting hyaluronidase. For these reasons, HAs have become the preferred fillers in the thin-skinned tear-trough region ( Fig. 18.1a,b ).
Other HA fillers available in the United States include Hydrelle (Anika Therapeutics, Bedford, MA), Prevelle Silk (Mentor, Santa Barbara, CA), and Puragen. Hydrelle (Anika Therapeutics), which has the highest concentration of HA per syringe at 28 mg/mL, was the first FDA-approved HA product to include lidocaine. Prevelle Silk also contains lidocaine and has an HA concentration of only 5.5 mg/mL, which provides a correction for 2 to 3 months. Puragen has a small particle size, improves flow characteristics, and reportedly can persist for 9 to 12 months.

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


