14 DeQuervain Tenosynovitis
Abstract
DeQuervain tenosynovitis (DQT) is a common cause of pain along the radial wrist, which can be treated successfully with nonoperative and operative care. The structures affected are the first dorsal extensor compartment tendons (the extensor pollicis brevis [EPB] and the abductor pollicis longus [APL] tendons). It can be related to traumatic or overuse activities, but frequently the pain occurs gradually and without obvious cause. Patients present with pain over the radial styloid aggravated by thumb movement. Conservative management is usually helpful and can consist of rest and activity modification, immobilization in a thumb spica brace, nonsteroidal anti-inflammatory medications (NSAIDs), and cortisone injection. If conservative care is not adequate, then surgery to decompress the first extensor compartment tendons is effective, safe, and reliable. Special attention is needed to look for and release a separate tunnel for the EPB tendon, to prevent volar subluxation of the tendons after the release, and to avoid injury to the branches of the radial sensory nerve.
14.1 Introduction
DeQuervain tenosynovitis (DQT) or disease is a common cause of pain and disability affecting the wrist. The complaint is pain along the radial aspect of the wrist. DeQuervain disease can affect people of all ages, but it is more common in those in the forties and fifties. Women may be affected up to six to ten times more commonly than in men. It also frequently affects the parents and caretakers of the newborn baby after pregnancy.
Although DeQuervain disease is more commonly called a tenosynovitis, the underlying pathophysiology is a stenosing tendovaginitis of the first dorsal extensor compartment of the wrist. Tendovaginitis describes the inflamed and thickened retinacular sheath. There typically is not significant proliferative inflammatory tissue.
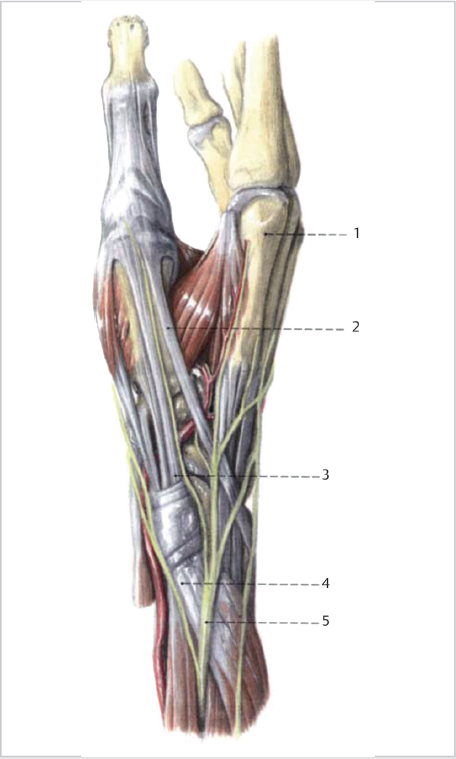
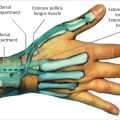
The first dorsal extensor compartment contains the EPB and APL (► Fig. 14.1). The average length of the compartment is 2cm. The distal edge of the compartment starts within 2mm of the tip of the radial styloid. Cadaveric studies show variations with the anatomy within the compartment. In more than 50% of wrists, there are multiple slips of the APL tendon, which insert into the trapezius and thenar muscles. The EPB is absent in 5 to 7% of cases. The most common arrangement is two slips of the APL and a single EPB (70%). Classically both tendons are found within a single tunnel, but two or more separate tunnels may be just as common. In one study a longitudinal septum was present in 47% of the specimens, and a separate EPB tunnel was found in 44%.
14.2 Evaluation
14.2.1 Patient History
The patient usually complains of pain in the radial aspect of the wrist. In addition there is often pain radiating proximally up the forearm, pain extending into the thumb, swelling, and occasionally feelings of crepitus or snapping with thumb motion. The pain is aggravated by activities that involve forceful and repetitive side-to-side motion with the wrist and by moving the thumb such as with pinching. Sometimes there is an acute specific cause such as a stressful activity. Lifting, carrying, and caring for a newborn baby are other common causes. But often the problem presents in a slow gradual fashion and is not related to any obvious history of traumatic or repetitive activities.
14.2.2 Physical Examination
The most common finding on physical examination is local tenderness to palpation and swelling around the radial styloid. Sometimes there may be an associated painful cyst growing in the region of the radial styloid. Eichoff maneuver is a provocative maneuver that is the hallmark for the evaluation of DQT. This test involves placing the thumb in the palm with the other fingers wrapped around the thumb in a clenched fist. This is followed by ulnar deviating the wrist. Pain with this maneuver indicates and is pathognomonic of DQT. The Finkelstein test, also used for the diagnosis of DQT, is a similar maneuver that involves grasping of the thumb and quickly abducting the hand ulnarward. The Finkelstein maneuver is commonly confused with the Eichoff test. The EPB entrapment test helps to differentiate pain arising from a separate EPB tendon compartment that may have gone unreleased during surgery. The examiner first applies resistance to isolated thumb metacarpophalangeal (MP) joint extension, then resists thumb palmar abduction. The test is positive when the pain produced by resisted thumb MP joint extension is more than that of resisted thumb palmar abduction.
14.2.3 Imaging
Routine radiographic imaging is not needed to diagnose DeQuervain disease. X-rays may be helpful if there is nearby pain in the carpus to evaluate for thumb carpometacarpal (CMC) arthritis, radiocarpal arthritis, calcific tendinitis, or occult traumatic injury.
14.2.4 Differential Diagnosis
Another common cause of pain along the radial wrist and hand is thumb CMC arthritis. But the location of the pain is separate and distinct from the pain in DeQuervain disease. Intersection syndrome usually causes pain and swelling more proximally along the radial wrist, and is associated with palpable and sometimes audible crepitation with flexion and extension of the wrist. Superficial radial nerve neuritis (Wartenberg syndrome or cheiralgia paresthetica) is usually associated with numbness over the dorsoradial hand.
14.3 Nonoperative Treatment
Conservative treatment options consist of rest and activity modification, immobilization in a thumb spica splint or brace, nonsteroidal anti-inflammatory medication (NSAIDs), and cortisone injection into the first dorsal compartment. Improvements with one or two cortisone injections have been reported in 60 to 80% of cases. In cases related to caring for a newborn, eventual improvement is usually expected with treatment and time. But repeated injections (more than two or three) may not be effective. In addition with the cortisone injections in this subcutaneous area of the wrist, there is a small risk of local skin complications including depigmentation, subcutaneous atrophy, and fat necrosis, particularly in darker-skinned individuals, which usually resolve within 1 year.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


