11. Venous Thromboembolism and the Aesthetic Surgery Patient
VTE is a life- or limb-threatening complication that can occur after surgical procedures.
It has been designated by the CDC as the most common cause of “preventable” hospital deaths and has been designated by the Centers for Medicare and Medicaid Services as a “never event” for some surgical procedures.
The annual estimate of VTE events is 500,000 cases with 100,000 deaths in the United States.
VTE occurs in 18,000 plastic surgery patients a year, and, although this may seem rare, it can be particularly devastating when it occurs in elective aesthetic surgery patients.
Surgeons should consider patients’ VTE risk as part of the standard aesthetic surgery workup.
Although research in plastic surgery patients has clearly demonstrated that all VTEs are not preventable, surgeons can minimize VTE risk preoperatively, intraoperatively, and postoperatively.
What do the Guidelines Say?
Both the American Society of Plastic Surgeons (ASPS) (2012) and American Association of Plastic Surgeons (AAPS) (2016) have published evidence-based consensus statements on VTE risk stratification and prophylaxis. 1 , 2
Both sets of recommendations advocate for individualized VTE risk stratification using the 2005 Caprini Risk Assessment Model (RAM). 3
Both sets of recommendations recommend different VTE prevention strategies based on baseline VTE risk, characterized by Caprini score and by procedure type.
A “one size fits all” approach is not recommended
Summary of Current Guidelines
The ASPS VTE Task Force 1 makes recommendations for aesthetic surgery patients who have surgery under general anesthesia. Direct quotes are provided from their 2012 manuscript.
Risk stratification: “Should consider completing a 2005 Caprini RAM…to stratify patients into a VTE risk category based on their individual risk factors”
For elective surgery patients with Caprini scores of ≥7: “Should consider utilizing risk reduction strategies such as limiting OR times, weight reduction, discontinuing hormone replacement therapy, and early postoperative mobilization”
For body contouring or abdominoplasty under general anesthesia with procedure time >60 minutes:
Caprini score 3-6: “Should consider the option to use postoperative low-molecular weight heparin or unfractionated heparin”
Caprini score ≥3: “Should consider the option to utilize mechanical prophylaxis… for nonambulatory patients”
Caprini score ≥7: “Should strongly consider the option to use extended (duration) low-molecular-weight heparin postoperative prophylaxis”
The AAPS published a systematic review/meta-analysis and consensus panel on DVT/PE prevention in 2016. Source data were largely derived from inpatient surgery, but several recommendations were applicable to the aesthetic surgery population. 2 Direct quotes are provided from their manuscript.
“We recommend using nongeneral anesthesia when appropriate. When possible, consideration should be given to using monitored anesthesia care, local anesthesia with sedation, or neuraxial anesthesia instead of general anesthesia.”
“We recommend using intermittent pneumatic compression to prevent perioperative VTE events in plastic surgery patients…intermittent pneumatic compression is superior to elastic compression stockings.”
“We recommend all plastic and reconstructive surgery patients should be risk stratified for perioperative VTE risk using a 2005 Caprini score.”
“We do not recommend adding chemoprophylaxis to intermittent pneumatic compression for VTE prophylaxis in the general non-risk-stratified plastic surgery population.”
“We recommend that surgeons consider chemoprophylaxis on a case-by-case basis in patients with Caprini score >8.”
“We do not recommend adding routine chemoprophylaxis for VTE prophylaxis in non-risk-stratified patients undergoing…body contouring.”
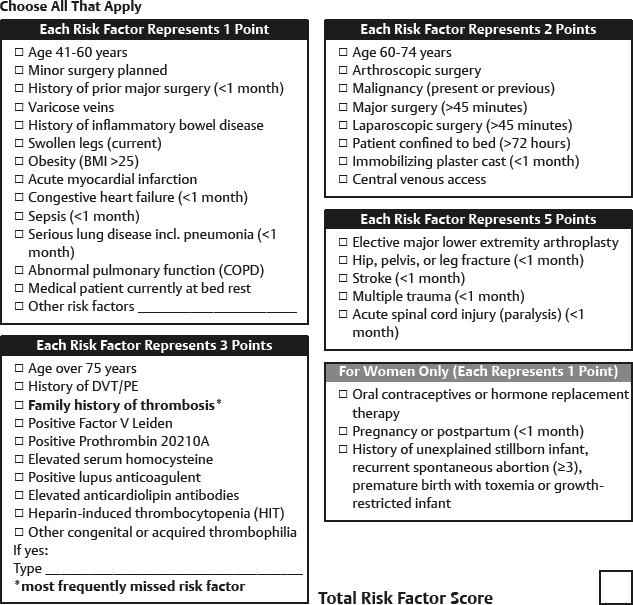
Understanding the Caprini Risk Assessment Model
This is a VTE risk assessment model that has been validated in >20,000 patients, including plastic, general/vascular/urology, gynecology oncology, and otolaryngology/head and neck.
The Caprini RAM is a one-page questionnaire that is easy to complete at either the patient’s initial consultation or preoperative visit (Fig. 11-1).
Assigns different point values for the various risk factors based on the patient’s personal medical history and family history.
An aggregate risk factor score is generated and correlates with a percentage value for postoperative VTE risk.
Using this information, physicians can make a decision about chemoprophylaxis an other risk-reduction strategies.
Current recommendations support the use of the 2005 Caprini RAM and not the 2010 Caprini RAM, which places more patients in a higher-risk category but does not increase the sensitivity of predicting VTE. 4
What Aesthetic Surgery Patients are at Highest Risk?
Among cosmetic procedures, abdominoplasty alone or in combination with another procedure has the highest risk of VTE. The procedure type with the greatest risk is circumferential abdominoplasty , which has an associated VTE frequency of 3.40%. 5
The Doctors Company has seen an increase in malpractice claims involving VTE, and a major issue is inadequate prophylaxis in high-risk patients.
In a review of 12 claims, 8 were abdominoplasty cases (6 of those 8 were combined procedures). Half of all patients had general anesthesia, the other half had IV sedation. Death occurred in 9 patients.
Why is the risk of VTE increased with abdominoplasty?
Multifactorial. Contributing causes include length of procedure (venous pooling with general anesthesia), prone positioning for hip liposuction (increased venous pressure from hip roll), fluid shifts with liposuction, increased intraabdominal pressure from rectus plication, flexed posture and postoperative abdominal binder, 6 and decreased postoperative mobility.
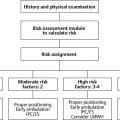
What Can Be Done Before Surgery—Risk Stratification
Complete a full history and physical examination and a VTE risk assessment tool such as the 2005 Caprini RAM. This tool reminds surgeons to ask about family history of VTE (the most commonly missed risk factor), genetic hypercoagulability, and current estrogen usage, among other often missed risk factors.
Note:
No VTE risk stratification tool has been validated for aesthetic surgery patients.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


