Abstract
This chapter examines the complicated and intricate process of wound healing, showing that the several phases of healing and wound types require a thorough understanding by plastic surgeons and practitioners in order to yield the most satisfactory outcomes. Wounds may move from an acute phase to the chronic type, requiring the physician to intervene in order to return these wounds back to a favorable phase of the healing cascade. With a multitude of surgical and nonsurgical options for treating wounds, the correct intervention may seem to be an overwhelming or daunting task. Accordingly, the authors stress the importance of education on wound healing pathophysiology and the available surgical and nonsurgical options. Each wound must be carefully evaluated, categorized, and finally treated.
1 Wound Healing: Science and Clinical Relevance
1.1 Goals and Objectives
Understand the wound healing pathophysiology.
Clearly define the characteristics of acute versus chronic wounds.
Appreciate the technical aspects of managing different types of wounds.
Know the evidence-based data on wound healing adjuncts.
1.2 Introduction
1.2.1 Overview
Wound healing is a complicated and intricate process, with several phases of healing and wound types, requiring a thorough understanding by plastic surgeons and practitioners alike to yield the most satisfactory outcomes. Wounds may move from an acute phase to the chronic type, requiring the physician to intervene in order to bring these wounds back into a favorable phase of the healing cascade. With a multitude of surgical and nonsurgical options for treating wounds, the correct intervention may seem to be an overwhelming or daunting task. The authors stress the importance of education on wound healing pathophysiology and the available surgical and nonsurgical options. Each wound must be carefully evaluated, categorized, and finally treated.
1.2.2 Clinical Challenge
Injury to the skin provides a unique challenge to clinicians, as wound healing is a complex and intricate process. With more than 6.5 million chronic skin ulcers caused by pressure, venous stasis, or diabetes mellitus, it is no wonder why cutaneous wound healing has become a topic of ongoing research and debate worldwide. 1 There are a multitude of options when considering adjuncts or primary treatment of these wounds. Cost-effectiveness is an important variable in treating these wounds, as chronic wounds account for an estimated $6 to $15 billion annually in U.S. health care costs. 2 There is tremendous pressure on the medical system and clinicians to develop cost-effective therapies.
There are a multitude of products available for the treatment of chronic wounds beyond the standard surgical debridement. Examples of these products include negative pressure wound therapy, hyperbaric oxygen, biologic dressings, skin substitutes, as well as growth factors and regenerative materials. The overwhelming amount of wound dressings and adjuncts available in the market implies a lack of full understanding of wound care and management. 3 The use of many of these adjuncts or materials is to improve upon specific wound characteristics to bring it as close to “ideal” as possible. It is vital for the clinician to have a thorough understanding of wound healing pathophysiology, wound characteristics, as well as the importance of surgical intervention before applying any of the advanced therapies.
1.2.3 Growth Factors, Cytokines, and Chemokines
Stanley Cohen’s experiment in which he noticed that the purification of submaxillary gland extracts led to earlier eyelid separation and eruption of the incisor in mice, eventually leading to the isolation of the first growth factor, epidermal growth factor (EGF), and the 1986 Nobel prize in Medicine. 4 It was after this discovery that knowledge of growth factors has increased rapidly. In only the past few decades, the discovery of growth factors has led to tremendous hope and speculation in regard to their use in the treatment of wounds, particularly difficult-to-heal or chronic wounds. The importance of growth factors, cytokines, and chemokines in regulating the complex process of wound healing has been studied extensively. 5 In vitro experiments have shown that growth factors are very effective in regulating cell proliferation, chemotaxis, and extracellular matrix (ECM) formation. Of particular importance is the EGF family, transforming growth factor-beta (TGF-β) family, fibroblast growth factor (FGF) family, vascular endothelial growth factor (VEGF) family, granulocyte macrophage colony-stimulating factor (GM-CSF), platelet-derived growth factor (PDGF), human growth hormone, and the interleukin (IL) family. It was not until further advances in recombinant technology became available that large amounts of purified growth factors could be obtained and tested in human clinical trials. Since this time, a large number of trials have been performed to evaluate the safety and effectiveness of growth factors in the healing of chronic wounds, including pressure, diabetic, and venous insufficiency–related wounds.
Currently, growth factors have a limited role in clinical practice. In the United States, recombinant human (rh) PDGF-BB (Regranex; Ortho-McNeil-Janssen Pharmaceuticals, Inc., Raritan, NJ) is the only growth factor approved by the U.S. Food and Drug Administration for use in chronic wounds. It has successfully completed randomized clinical trials in the United States and is available as a commercial product. In this brief discussion, we will review wound-healing mechanics and considerations in treatment, and mention different modalities for treatment. The discussion will be ended with a perspective on the future of growth factors in chronic wounds.
1.3 Wound Healing Pathophysiology
Wound healing involves a complex set of simultaneous processes including activation of the inflammatory cascade, vascular neogenesis, and cell proliferation. It is a set of interactions that is still poorly understood.
With regard to cutaneous wound healing, scarring is the body’s attempt at reestablishing homeostasis and preventing infection. The tissue laid down in scarring is inherently different than the skin that it replaces. Therefore, scarring is different from wound healing of other organs, such as the liver or bone, or that which occurs in fetal wound healing, which heals by regeneration and re-creation of the same previously existing tissue. It is critical to understand the differences in these healing processes, as well as the progression of each, so that we can determine where we may intervene clinically to alter the body’s response.
There are three phases of wound healing that are generally cited: inflammation, proliferation, and remodeling phases (Fig. 1‑1). While devitalized tissue is removed during the inflammatory phase, new tissue is laid down in the proliferative phase, and finally the structure of the scar is optimized during the remodeling phase. The primary goals of the inflammatory phase are ridding the newly created wound of bacteria and dead tissue. At the same time, hemostasis is achieved. When the wound is initially created, there are several processes occurring at the same time including creation of a provisional matrix, release of cells and growth factors from ongoing hemorrhage, and initiation of the clotting cascade. These processes are interactive: as platelets clump to achieve hemostasis, they also release PDGF and TGF-β). Exposed collagen and tissue factor from the initial injury begin the clotting cascade, which ends in the formation of a fibrin-based matrix. Inflammatory cells and growth factors attach to this scaffold to create the proper milieu for subsequent wound healing.
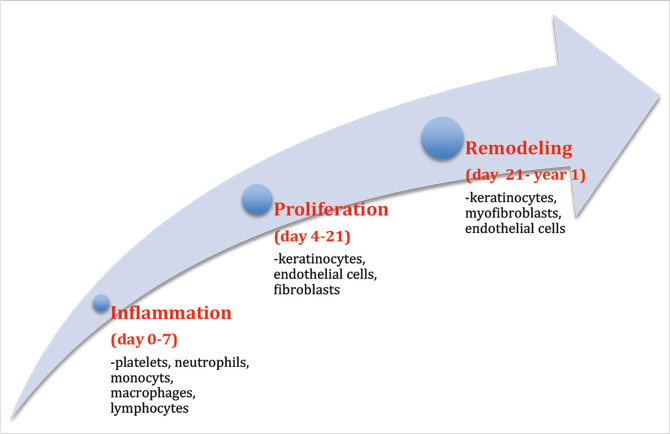
Inflammatory cells are attracted to the wound by TGF-β from platelets, lipopolysaccharide from bacteria, and elements of the clotting cascade. 6 Neutrophils permeate the wound in the first 48 hours to remove dead tissue and destroy bacteria. Monocytes enter the wound at 48 to 72 hours and become phagocytosing macrophages. Interestingly, wound healing cannot progress without the presence of macrophages, but it is able to progress without neutrophils. 7 , 8 Lymphocytes enter the wound at days 5 to 7. Their role is not well defined, but they may initially play a role in the proliferative phase of wound healing. 9
During the proliferative phase of wound healing, re-epithelialization and granulation tissue formation occur. This generally occurs from days 4 to 21 after injury. The provisional matrix that was formed in the inflammatory phase is replaced by ECM with type III collagen and blood vessels of new granulation tissue. Macrophages release cytokines that stimulate fibroblasts to lay down this new ECM and endothelial cells form these new blood vessels. Eventually, as the proliferative phase comes to an end, the fibroblasts and blood vessels regress, although we require further research into the regulation of this process.
The remodeling phase is characterized by the replacement of type III collagen with type I collagen, as well as wound contraction by myofibroblasts. The wound strength changes over the course of the remodeling phase. Wounds have only 20% strength of normal skin at 3 weeks after injury, and will reach 70 to 80% strength of normal skin at 1 year.
1.4 Acute versus Chronic Wounds
Wounds that fail to progress through the normal stages of healing become chronic wounds. An acute wound is one that is present up to 3 weeks, while a chronic wound is one that has been present for greater than 2 to 3 weeks. These chronic wounds remain a significant challenge and burden on U.S. healthcare. Chronic wounds including venous stasis ulcers, decubitus ulcers, and diabetic foot ulcers affect over 6 million people in the United States. Despite treatment, the recurrence of these wounds is high and costs the healthcare system billions of dollars each year. 10
Before determining treatment for a chronic wound, it is important to elucidate the history of the wound and contributing risk factors. Factors that delay wound healing include infection, ischemia, smoking, necrotic tissues, venous stasis, edema, diabetes, and steroids.
1.5 Factors Affecting Wound Healing
Wounds are more susceptible to healing in a moist, clean, and warm environment. A moist wound bed will allow growth factors and various cell types to migrate, facilitating wound edge contraction. In order to create and maintain this environment, appropriate dressings come into play as outlined in the following section.
Bacterial contamination of wounds can prevent the normal phases of wound healing from taking place by virtue of effects on inflammation or by secretion of active proteases. For example, platelet aggregation and hemostasis can be affected by bacteria. 11 Leukocyte function is impaired by bacterial virulence factors and length of inflammation is prolonged. 12 The formation of granulation tissue may be impaired by the presence of bacteria. 13 Not all bacterial species are equal in their ability to retard wound healing: beta-hemolytic streptococcus can produce wound healing complications at lower levels than other organisms. 11
With regard to ischemia, in vitro studies have demonstrated that neutrophils and fibroblasts do not function appropriately at low oxygen levels. 14 , 15 Clinically, low subcutaneous oxygen tension of a wound has been shown to be a predictor of surgical wound infections. 16 Therefore, it is critical to optimize bloody supply, especially if the upper or lower extremity is affected. Revascularization should be considered prior to any advanced surgical procedures, although a debridement may be necessary earlier. Similarly, venous stasis ulcers should be accompanied by compression therapy along with debridement to optimize the outcome. Interestingly, although tissue perfusion appears to be critical to wound healing, low hemoglobin levels are not the normal physiologic responses to anemia tend to restore normal oxygen delivery despite low hemoglobin levels. 17 , 18
Among the components of cigarettes that can impair wound healing are nicotine, carbon monoxide, and hydrogen cyanide. 19 In addition to being a vasoconstrictor, nicotine increases platelet aggregation, and impairs the proliferation of red blood cells, fibroblasts, and macrophages. Carbon monoxide impairs oxygen transport and metabolism, while cyanide inhibits oxidative metabolism. The complications of wound healing in plastic surgery caused by smoking are well documented in patients having facelifts, breast reduction, breast reconstruction, and abdominoplasty. 20 , 21 , 22 Despite the clear benefits of smoking cessation in surgical patients, the time period for cessation is unclear. Some have recommended smoking cessation 4 weeks prior to surgery, and 4 weeks after surgery. 23
Diabetes can affect wound healing at both the macro and micro levels. Diabetes is known to cause vascular disease impairing blood flow and oxygen delivery to tissues. 24 Hyperglycemia results in protein and enzymatic dysfunction leading to inflammation. 25 In addition, hyperglycemia results in alteration of basement membrane permeability. Again, recommendations for perioperative glycemic control are unclear, but those patients with levels greater than 200 mg/dL generally have worse outcomes. 26
Steroids have been shown to impair epithelialization, collagen formation, and the inflammatory process. The effect on wound healing is likely clinically apparent only when taken chronically within 30 days of surgery; steroids taken in the acute phase likely have little effect on wound healing. 27 In contrast, although chemotherapeutic drugs would logically impair wound healing based on their ability to impair nucleic acid and protein synthesis, as well as cell division, clinical studies have not borne this out. 28 Radiation causes DNA and protein damage, vascular stasis and thrombosis, impaired fibroblast activity, and in addition may cause clinically significant changes including slower epithelialization, decreased tensile strength, and higher dehiscence rates. 29 , 30 , 31
Examination of chronic wounds should include depth of the ulcer, size, presence of cellulitis, and other signs of infection. Measurements should be performed weekly to determine healing progress. Decrease in wound size of 10 to 15% per week indicates potential for normal healing. Gentle probing may be utilized to determine if bone is present at the base of the wound. If bone is present, there is a high likelihood of osteomyelitis. A thorough neurovascular exam should be documented including pulses, Doppler examination, and sensation using Semmes-Weinstein filaments. 10
1.6 Surgical Intervention and Debridement
After appropriate assessment of a wound, it may be deemed appropriate for a variety of debridement options: autolytic, enzymatic, mechanical, or even larval therapy. Nonetheless, surgical debridement, or mechanical, remains a mainstay in the treatment of chronic or hard to treat wounds (Fig. 1‑2). Through wound bed preparation, even complicated wounds may effectively turn into acute wounds and proper cellular responses induced to allow healing. If surgical intervention is to be performed in an attempt to convert a chronic wound to an acute one, nonviable tissue should be debrided thoroughly until healthy, bleeding tissue is encountered. Multiple debridements may be necessary if the extent of nonviable tissue is not clear initially. The use of hydrosurgery devices has advanced the surgical management of wounds, as it has become an option that can control the depth of tissue removal more precisely, and therefore spare more healthy tissue while still achieving adequate debridement. 32 Debridement of skin should be continued until pinpoint-bleeding tissue that blanches is encountered. Healthy fat will appear soft and shiny, while fascia and tendon that is healthy will appear shiny and taut. Healthy bone will be firm with cortical bleeding. 10 Tissue cultures should be sent for any debrided tissue.

1.7 Wound Dressings and Healing Adjuncts
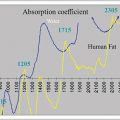
As discussed previously, wounds are more prone to healing in a moist, clean, and warm environment. There are four basic principles involved when choosing an optimal dressing type. If a wound is dry or desiccated, it will need hydration. If a wound produces excessive exudates, the fluid needs to be absorbed or removed (Fig. 1‑3). If a wound has necrotic tissue or evident debris, it will need a debridement. Lastly, if a wound is infected, it will need to be treated with the appropriate antibacterial agent. Other factors also important in choosing a dressing include providing protection to the peri-wound skin, forming an effective bacterial barrier, conforming to wound shape, producing minimal pain during application and removal, being free of toxic or irritant extractables, not releasing particles or non-biodegradable fibers into the wound, and maintaining the wound at an optimal temperature and pH. Each wound needs a proper assessment of its characteristics and these needs can be met with a corresponding dressing that fits the situation. It is important to remember that wound environments change and dressings should be changed accordingly.

Box 1.1 Characteristics of an Ideal Dressing
Creates a moist, clean, warm environment.
Provides hydration if dry or desiccated.
Removes excess exudates.
Prevents desiccation and is nontraumatic.
Provides protection to the peri-wound area.
Allows for gaseous exchange.
Impermeable to microorganisms.
Free of toxic or irritant particles.
Can conform to wound shape.
Minimal pain during application and removal.
Easy to use.
Cost-effective.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


