Abstract
This chapter looks at the subjective quality of beauty through a scientific lens. Facial aesthetics are addressed in detail, along with the various factors that affect facial beauty—aging, skin and soft tissue, and skeletal support. Considerations in the preoperative evaluation are covered that will assist the surgeon in the aesthetic assessment of the face. The components of symmetry, height, and width are discussed in relation to frontal and lateral view, midface and lower face analysis and projection. Each section of the face—the upper third, including forehead and eyebrows, the middle third, with the cheeks, nose, ears, and the lower third, the region of the mouth and lips—is thoroughly reviewed with respect to the governing principles, effects of aging, and management of remedial treatments. Finally, the chin and neck are introduced and common problems briefly reviewed.
6 Principles of Facial Aesthetics
6.1 Goals and Objectives
Understand principles of facial aesthetics through historical and surgical perspectives.
Describe anatomic changes associated with facial aging.
Apply principles of facial aesthetics to the aging face.
Understand the evaluation of prospective aesthetic patients seeking facial rejuvenation.
Describe various surgical and nonsurgical options to achieve the goals identified during consultation.
6.2 What Is Beauty?
Beauty has inspired, influenced, and captivated humans throughout time. For thousands of years, we have attempted to understand, define, and depict beauty in art, literature, architecture, nature, and human form. But what is beauty? In the broadest sense, beauty can be defined as the combination of qualities pleasing the aesthetic senses. Attractive faces activate the reward centers in the brain, elicit the development of human relationships, motivate partner selection, and activate positive treatment in many social settings. 1 , 2 Attractive people are more likely to be hired for jobs, to be promoted, to wait shorter periods of time for services, are less likely to be reported or punished for crimes, are more likely to have dates, and are perceived to possess positive personality attributes such as kindness and honesty. 3 , 4 , 5 , 6
Although the positive social consequences of facial attractiveness have been well studied, determinants of features that define an attractive face remain poorly understood. If standards for facial beauty are learned and influenced solely by individual preference, culture, and era, then what is perceived as beautiful would vary dramatically across time and space. However, regardless of age, nationality, ethnicity, culture, or era, people share a sense of what is attractive. Several cross-cultural studies support the hypothesis that the perception of beauty is uniform across culture. 7 , 8 , 9 , 10 When presented with attractive and unattractive faces, masks, or dolls, infants gaze at the attractive face for a longer period of time and prefer attractiveness to symmetry. 11 , 12 , 13 The emergence of preferences for beauty in early human development and cross-cultural agreement challenges the argument that beauty is defined exclusively by culture and supports the notion that our preferences may be biologically determined by natural selection. 14 But what is ideal for beauty?
Preferences for symmetry are likely to be an evolutionary trait that serves as a surrogate marker for phenotypic and genetic fitness. Asymmetry is a consequence of normal aging and is perceived as less attractive compared to a symmetric face. Averageness, or how closely a face resembles the majority in the population, is also considered attractive. 15 , 16 , 17 , 18 It is important to note, however, that extreme beauty is associated with magnification or diminution of a specific feature. For a male, this could mean an augmented dominant feature, such as a prominent chin. Individual characteristics that deviate from the average can increase attractiveness and should be considered when addressing the patient’s aesthetic goals.
It is also important to consider physical characteristics that differ among men and women. In studies involving facial composite photographs, females often preferred men with more masculine features such as deep-set and small eyes, large, wide, and square jaws, prominent chins, thin lips, and facial hair; on the other hand, males preferred females with large foreheads, large eyes, prominent cheekbones, a small nose, small chin, and full lips. 19 , 20 , 21 In males, this corresponds to a larger nasofacial angle and smaller nasomental, nasofrontal, and mentocervical angle compared to females. A high eyebrow position and a wide smile were considered attractive “expressive” features of both sexes, suggesting high sociability.
Aesthetic principles must be considered in the context of ethnicity. Fitzpatrick skin type, scarring, and the ability to hide facial incisions vary widely among ethnic groups. Although certain facial proportions are constant throughout ethnicities, westernized principles of facial aesthetics cannot be applied to all since many patients desire to retain certain ethnic features. In contrast, certain well-publicized ethnic features are appealing to other groups, such as the very popular double eyelid blepharoplasty in the Asian population. Our concept of beauty will continue to evolve as we further understand facial harmony and standards of beauty among distinct ethnicities and as the concept of beauty continues to evolve with the increased global heterogeneity of ethnic backgrounds.
6.3 A History of Beauty
While beauty was idealized even in ancient cultures, it was not until the Greek philosophers began to study beauty that it became a discipline. The Greek philosopher and mathematician Plato described the ideal face with symmetry, proportion, harmony, and geometry in his “golden proportions,” where the width of the face would be two-thirds its length and the nose would be no longer than the distance between the eyes. In his text the Elements, Euclid defined the golden ratio, phi, which is equal to approximately 1.1618. The golden ratio, also called the divine ratio, is the only mathematical relationship consistently found throughout beautiful and harmonic things in nature, art, history, architecture, and the human form and face. This ratio is obtained when a line ABC is cut so that AB/AC = BC/AB (Fig. 6‑1). Phi has been studied extensively in facial aesthetics and utilized to derive a golden mask or ideal facial proportions. 22 , 23 While the mask may be an inexpensive and easy tool for facial analysis, the proportions are thought to be inconsistent and too masculinized for generalization. 24 , 25 Variations have been proposed, but recent studies utilizing three-dimensional stereophotogrammetry for facial anthropometry suggest that the ratios between facial distances were not related to attractiveness or the golden ratio. 26 , 27 Smaller faces and uniform facial thirds and fifths are thought to be more ideal ratios for females. 28
Other Greek figures also helped in defining ideal beauty of the human body, including the sculptors Polykeitos and Praxiteles who developed canons of physical proportions of the ideal body through their art. The Roman architect Vitruvius produced a facial trisection that is still used today by medical professionals. Today, we still utilize the Vitruvian thirds with some modification. 29 During the Renaissance, the ideal representation of facial form was revisited. Leonardo da Vinci exemplified anatomical ideals with geometric principles through the Vitruvian Man and also formulated the ideal facial proportions of vertical fifths. Vitruvian principles also influenced the German printmaker Albrect Durer, who published a four-book series on human proportion in 1528.
Facial aesthetics largely depend on the three-dimensional topography of the central features of the face, namely, the eyes, nose, cheeks, and lips. Cephalometry was introduced in the early 18th century to quantitatively understand the growth, development, and relationship of skeletal structures. Anthropometric methods utilize surface topographic measurements and are preferable to cephalometric methods in determining ideal facial proportions. Anthropometry provides simple, non-invasive, comprehensive three-dimensional population-matched data. Powell and Humphreys provided a detailed analysis of facial contours, angles, and proportions in their 1984 text Proportions of the Aesthetic Face. 30
6.4 Facial Aging
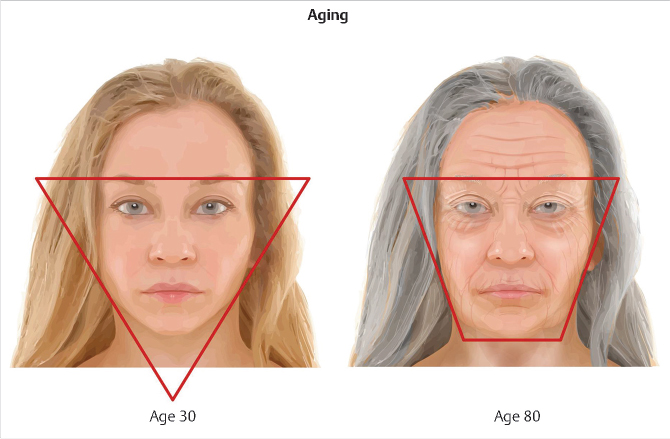
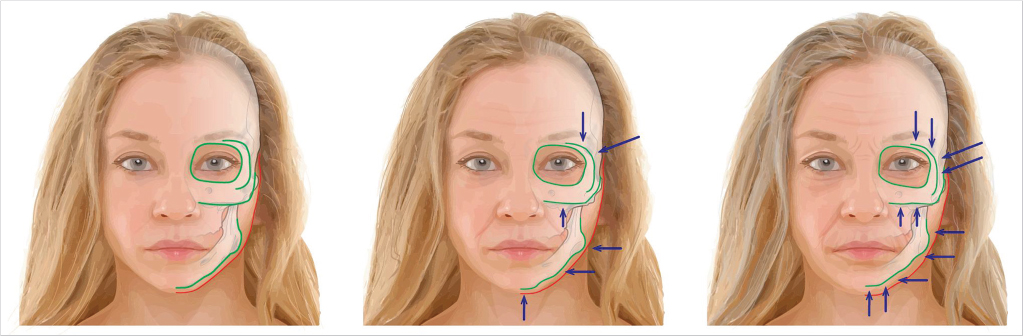
Facial aging reflects the cumulative, dynamic, and interdependent structural changes of the skin, soft tissues (subcutaneous fat, muscle, fascia, and ligamentous structures), and structural support (bone and teeth) of the face, leading to changes in facial volume and topography (Fig. 6‑2). 31 There is a general descent of the soft tissues with age, which has been described by an inverted triangle (Fig. 6‑3).

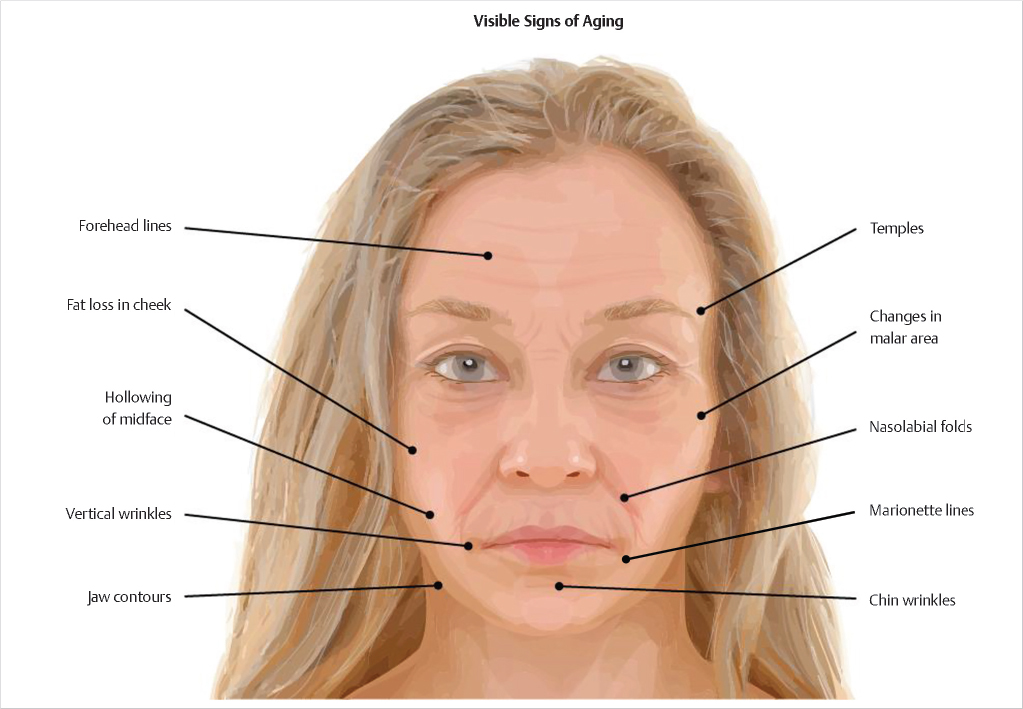
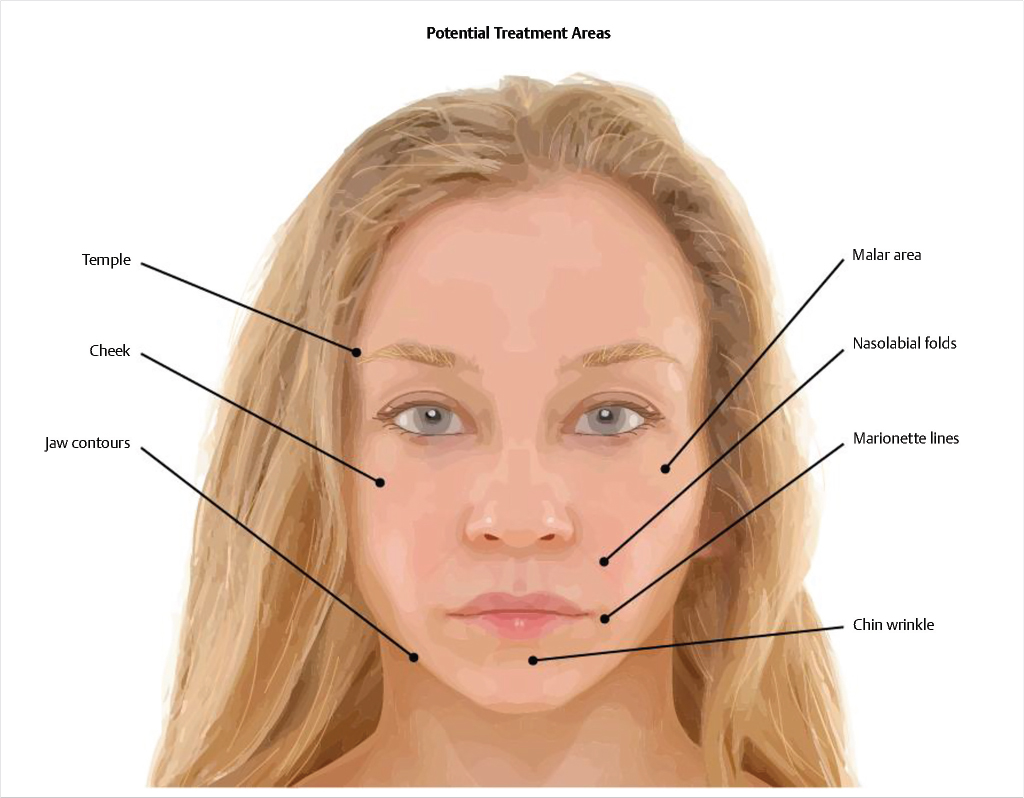
The factors contributing to facial aging are multifactorial and can be due to the effects of genetics, gravity, photoaging, medical comorbidities, diet, chronic smoking or alcohol use, large changes in weight, stress, environmental factors, decreased tissue elasticity, craniofacial remodeling, subcutaneous fat redistribution, and other factors. The visible signs of aging can include features such as horizontal and vertical rhytids, temporal atrophy, volume loss in the midface, deep nasolabial folds, and jowls (Fig. 6‑4) areas all of which are amenable to treatment (Fig. 6‑5).
6.5 Skin
Aging skin results from deterioration of the skin’s structure and function and is associated with changes in the epidermis, dermis, and subcutaneous layers. Factors contributing to the appearance of aged skin include dry and thin skin, a dull and rough complexion, enlarged pores, irregular pigmentation, actinic keratosis, loss of firmness and elasticity, broken blood vessels, fine lines, and deep wrinkles. There are three main types of aging responsible for the change in the structure, function, and quality of the skin.
Biological (intrinsic): chronological age, genetics
Environmental (extrinsic): sun exposure, pollution, cigarette smoke, or external stress such as dry cold weather
Mechanical: repeated muscle contraction
In the epidermis, decreased cellular turnover, reduced keratinocytes and epidermal lipids, and decreased moisture result in dry skin. Altered pigmentation results from fewer melanocytes and melanin production. In the dermis, reduced repair and turnover and reduced function of the sebaceous and sweat glands cause dry skin. Histologically, there are fewer fibroblasts and collagen production, reduced dermal matrix, and thicker elastin fibers with less elasticity. The blood vessels become thin, dilated, and weak. The thinning subcutaneous tissue and weakening retaining ligaments cause the skin to sag.
Management: Treatment of aging skin includes sunscreen, moisturizers, tretinoin, fillers and injectables, lipotransfer/autologous fat grafting, peeling and microdermabrasion, radiofrequency, and laser resurfacing.
6.6 Soft Tissues
The youthful face has an adequate volume and distribution of fat in specific areas. In the aging face, the forehead, temporal, periorbital, malar, glabellar, perioral, and mandibular sites lose fat, while the jowl, submental area, nasolabial folds, and infraorbital areas gain fat (Fig. 6‑6). 32 Contour deficiencies become increasingly apparent with the redistribution or atrophy of fat with age, and the defining convexities of the youthful face are lost. 33 Imaging studies reveal that the midfacial fat compartments migrate inferiorly with aging. Retaining ligaments that provide support to the soft tissues and skin of the face, such as the anterior platysma-cutaneous ligaments and mandibular osteocutaneous ligaments, become less supportive.

6.6.1 Management
Procedural rejuvenation techniques include non-invasive, minimally invasive, and invasive procedures, ranging from medical rejuvenation with retinols and alpha-hydroxy acids to procedural rejuvenation with laser resurfacing, botulinum toxin A, fillers, and radiofrequency all the way to surgical interventions such as liposuction or fat grafting, implants, and rhytidectomy.
6.7 Structural Support
Aging of the craniofacial skeleton is due to dynamic changes involving bone expansion and bone loss (Fig. 6‑7). 34 Specific changes in the facial skeleton which occur with aging include reduced facial height due to changes in the maxilla and mandible, increased facial width and depth, and increased prominence of the frontal sinus and zygomatic arches. Bony resorption leads to alteration of the structural support of bone and consequently alters overlying soft tissue and skin.
Management: Patients may present for consultation for problems such as midface hypoplasia, prominent zygoma, or square mandibular angle. The size, shape, balance, and proportion of the craniofacial skeleton can be manipulated through segmental osteotomies, genioplasties, mandibular angle reductions, malarplasties, and orthognathic surgeries to alter facial projections and aesthetics. 35
6.8 Preoperative Evaluation
Goals of the consultation should include an assessment of the patient’s objectives, perceptions, and expectations. This includes a consideration of personal preference, gender, cultural differences, and racial background. The goals of facial analysis should be to diagnose and classify deformities or deviations, develop a treatment approach, and predict outcomes. The risks, benefits, costs, side effects, potential adverse events, and anticipated outcomes should be thoroughly reviewed, and any of the patient’s questions should be answered.
Preoperative anteroposterior and lateral and oblique photographs assist the surgeon in planning, facilitate patient preoperative and postoperative discussion and review, and should be done for medicolegal documentation.
6.9 Facial Proportions and Aesthetic Assessment
Many methods have been utilized for assessment of the aesthetic units of the face and for determining their relationship and relative proportions in evaluating the face as a whole. Although no algorithm exists for aesthetic assessment of the face, systematic evaluation and preoperative facial measurements may aid in the determination of which facial features need to be altered in order to produce the best harmony.
Hom and Marentette developed an 8-step systematic approach to facial analysis. 36 The initial assessment should begin with an analysis of facial symmetry, height, and width on frontal view. Next, evaluation continues on profile to determine facial projection and the relationship between structures such as the forehead, nose, lip, and chin. Finally, individual subunits are carefully evaluated.
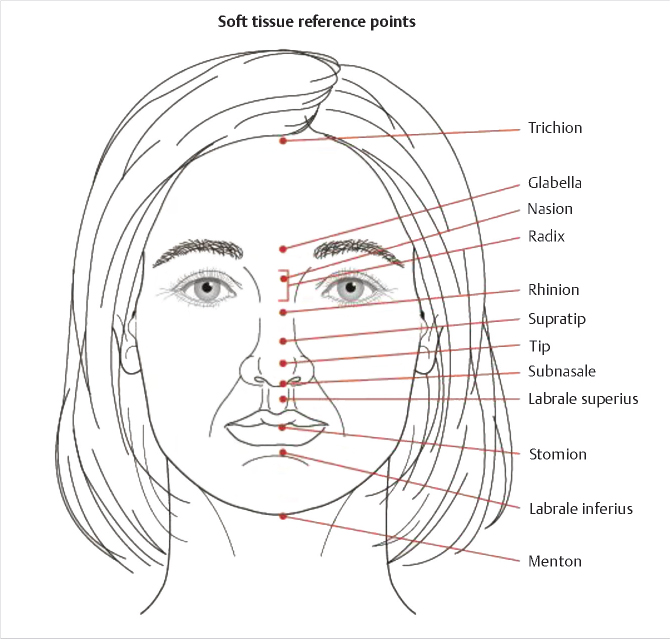
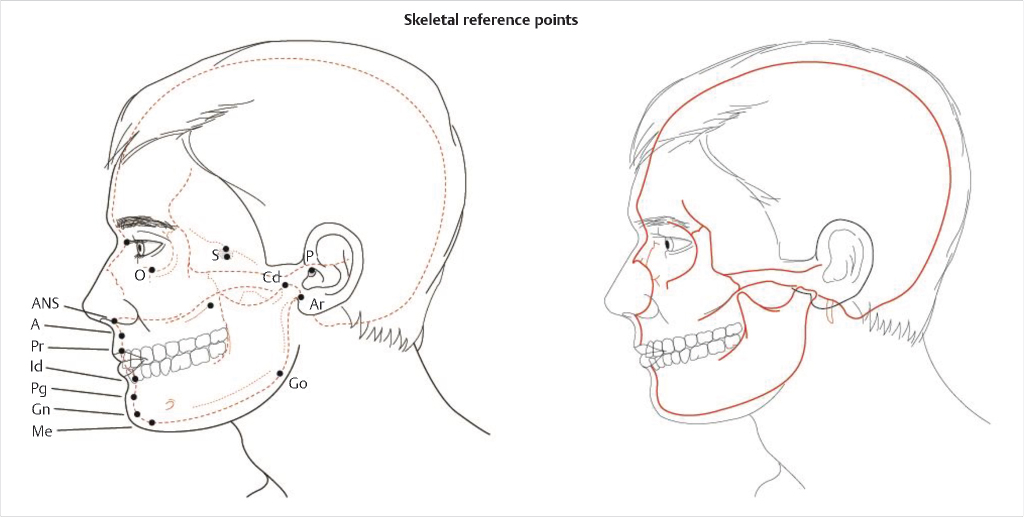
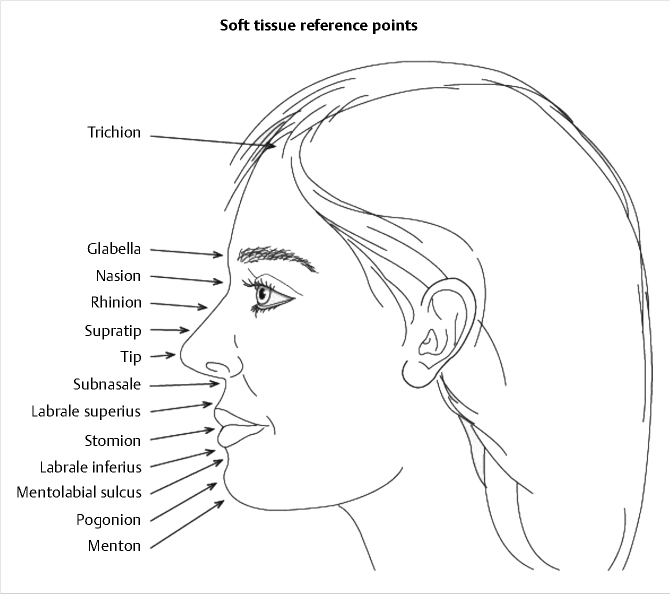
Facial analysis is dependent on the assessment of both soft tissue and the underlying craniofacial framework. Soft tissue reference points (Fig. 6‑8), skeletal reference points (Fig. 6‑9), and reference planes are defined by cephalometric analysis. Important elements in cephalometric analysis include maxillary, mandibular and incisor positions, and facial proportions. The Frankfort horizontal plane is the standard reference for patient positioning in photographs and cephalometric radiographs. This plane is defined as a line drawn from the superior portion of the external auditory canal (approximately at the level of the superior edge of the tragus) to the inferior border of the infraorbital rim when the patient’s gaze is parallel to the floor.
6.10 Frontal View Analysis
6.10.1 Symmetry
Aesthetic facial analysis can begin with a general evaluation for symmetry by bisecting the face with a midsagittal plane and comparing the halves, although symmetry is rarely perfect. The forehead, nose, lips, and chin should lie along this axis.
6.10.2 Height
Facial height is determined by dividing the face into equal horizontal thirds (Fig. 6‑10). The boundaries are from the trichion to the glabella (upper face), from the glabella to the subnasale (middle face), and from the subnasale to the menton (lower face). With a receding hairline, the most superior border of the upper third can be determined by identifying the most superior movement of the frontalis muscle.
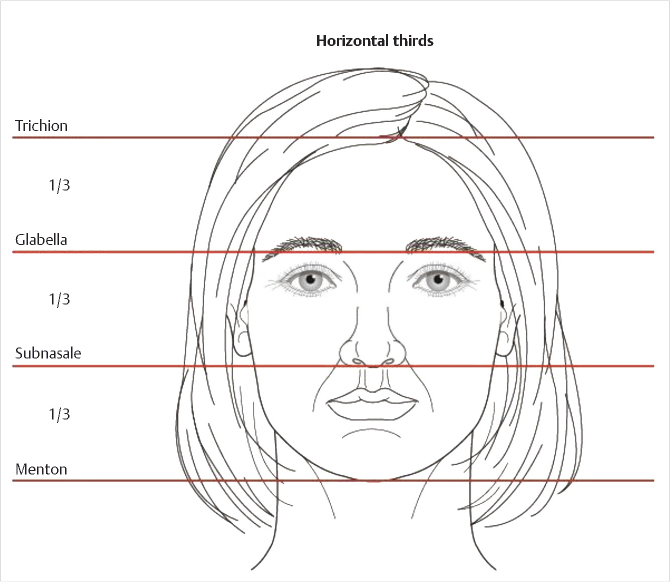
A second method for assessing facial height takes into consideration only the middle and lower portions of the face. The first measurement is from the nasion to the subnasale and from the subnasale to the menton. With this measurement, the midface is 43% of the total length and the lower face is 57% of the total length. This technique is advantageous since the nasion is a more reproducible landmark than the glabella.
6.10.3 Width
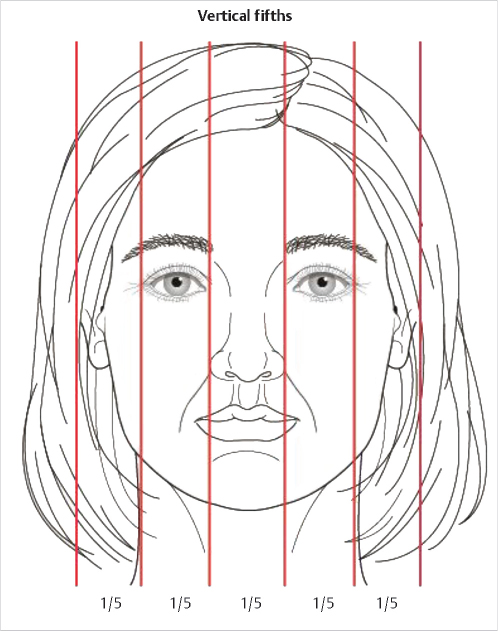
Facial width is then divided into equal fifths to evaluate balance among the parts (Fig. 6‑11). The width of one eye opening should equal one fifth of the facial width and this in turn is the width of the intercanthal distance. The lateral fifths on frontal view extend from the lateral canthus to the lateral portion of the helical rim.
6.11 Lateral View Analysis
6.11.1 Height
Facial height is assessed using the same landmarks described previously (Fig. 6‑12). In addition, the lower third can be further subdivided into thirds with the stomion separating the upper and middle thirds and the pogonion located in the center of the lower third.
6.11.2 Midface Projection
To assess the relationship of the midface with the upper face, a line is drawn from the nasion to the subnasale. The angle formed with the Frankfort horizontal line should be a right angle on average (Fig. 6‑13).
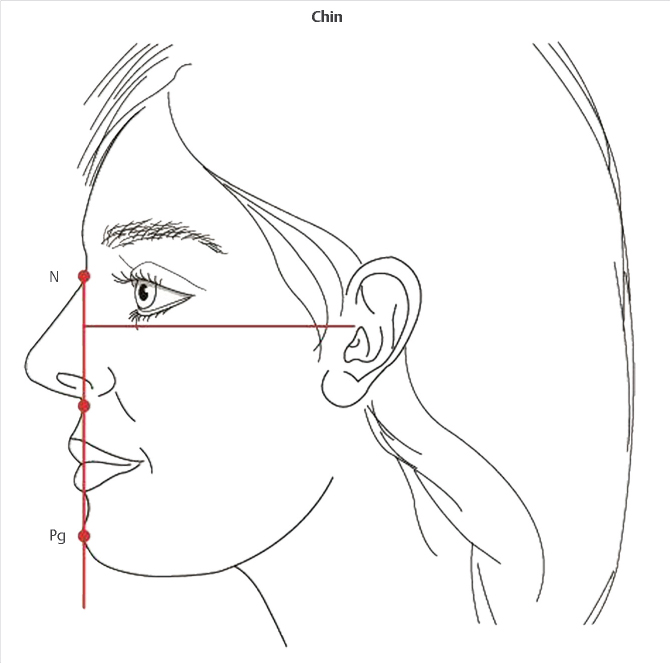
6.11.3 Lower Face Projection
To assess the relationship of the lower face to the midface, a line is drawn from the subnasale to the pogonion perpendicular to the Frankfort horizontal line. If the pogonion is posteriorly positioned, the chin is retruding; if it is anteriorly positioned, the chin is protruding (Fig. 6‑13).
6.12 Facial Aesthetic Units
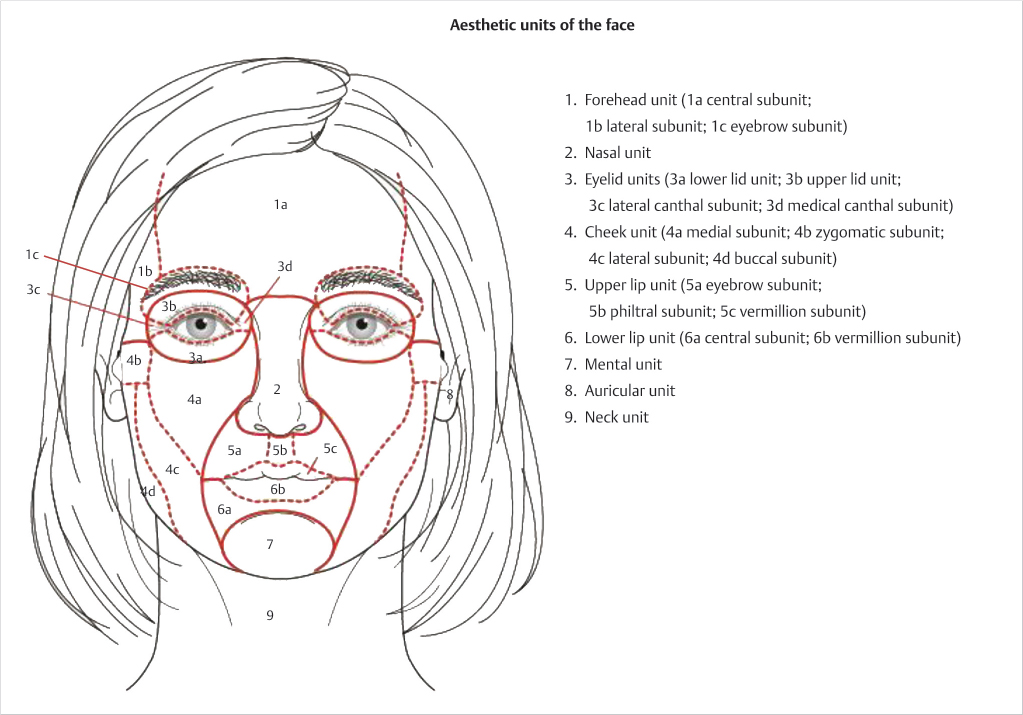
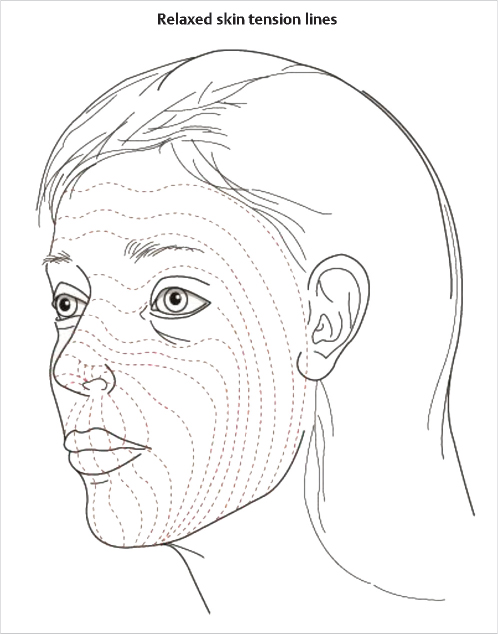
The face can be further divided into aesthetic units for further analysis: forehead, nose, eyelid, cheek, lips, chin, ears, and neck (Fig. 6‑14). The units of the face are evaluated for contour, texture, skin thickness, and color. Incisions that fall along relaxed skin tension lines and at the intersection of the aesthetic units result in the least noticeable and most favorable scars (Fig. 6‑15).
6.13 Upper Third
6.13.1 Forehead and Eyebrow
Principles
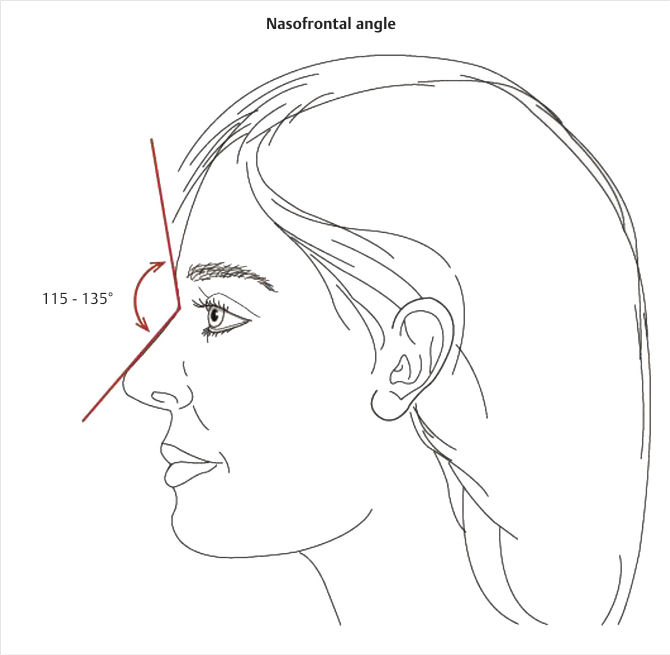
The forehead constitutes the entire upper third of the face and is convex on profile with the most anterior point above the nasion at the level of the supraorbital ridge. The boundaries of the forehead are from the frontal hairline to the glabella. In general, men have a more prominent glabellar and supraorbital rim compared to women due to larger, more aerated frontal sinuses. Women tend to have a rounder, more convex forehead. The nasofrontal angle is determined by a tangent passing through the glabella and nasion and a tangent along the nasal dorsum; this angle ranges from 115 to 135 degrees which allows for a wide variation that is gender-, ethnic- and age-related (Fig. 6‑16). The layers of the forehead and scalp region are skin, subcutaneous tissues, aponeurosis, loose areolar tissue, and periosteum, which can be remembered by the acronym SCALP. The galea aponeurosis connects the bellies of the frontalis and occipital muscles; laterally, it thins to become incorporated into the superficial temporal fascia.
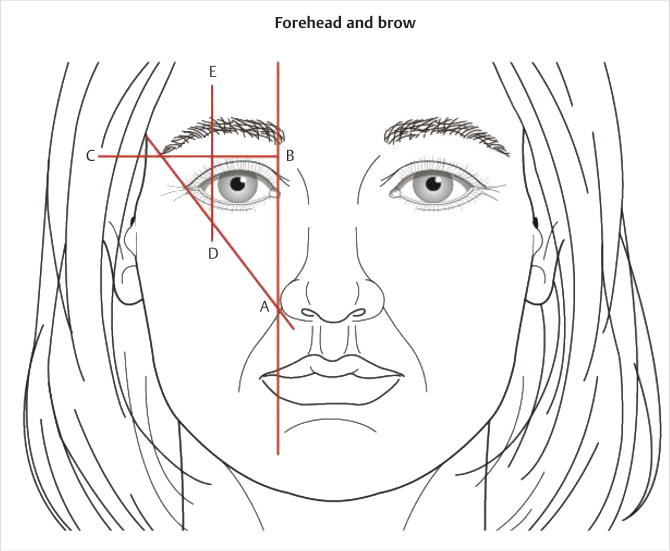
The female eyebrow is generally located 1 cm above the superior orbital rim and has a more prominent arch (Fig. 6‑17). The male eyebrow is located approximately at the level of the rim and is flat. The eyebrow extends medially to a position delineated by a vertical line drawn superiorly perpendicular to the alar base. The lateral aspect of the eyebrow is delineated by an oblique line drawn from the lateral aspect of the alar base through the lateral canthus. The medial and lateral ends of the eyebrow should be located at the same horizontal position. The apex of the eyebrow is delineated by a line drawn vertically from the lateral aspect of the corneal limbus.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


