Fig. 6.1
Patient’s trunk with xerosis, with fine scale and several nummular patches of mild erythema

Fig. 6.2
Patient’s foot with xerosis and fine scale

Fig. 6.3
Patient’s calf with xerosis and fine scale

Fig. 6.4
Patient’s ankle and lateral lower leg, with mild xerosis

Fig. 6.5
Patient’s upper back with mild xerosis, coexistent excoriations, hypopigmented scars consistent with previous trauma from pruritis

Fig. 6.6
Patient’s leg with chronic photodamage and xerosis
Differential Diagnoses
The differential diagnoses includes ichthyosis, atopic dermatitis, exfoliative dermatitis, asteatotic dermatitis, or any process that causes dry skin, including inadequate use of emollients. Ichthyosis can be acquired or inherited in an autosomal dominant or recessive fashion. Ichthyosis vulgaris is the most common form of ichthyosis and presents with fish-like scale sparing flexural surfaces. Atopic dermatitis tends to be stimulated by irritants such as food or environmental allergens, leading to itchiness, redness, and scaling; skin of the anticubital fossa, popliteal fossa, feet, ankles, hands, wrists, upper chest, neck, face, and eyelids tend to be affected. Although atopic dermatitis is seen in all ages with varying symptoms correlated with age, it is most prevalent in younger patients, particularly infants and children. Exfoliative dermatitis or erythroderma may result from drug therapy, systemic or cutaneous disease, or idiopathic causes, and manifests as generalized erythema and scaling affecting almost the entire body. Asteatotic dermatitis is most commonly seen in elderly patients, as a result of decreased sebaceous and sweat gland activity, and tends to affect the shins, hands, and trunk. It can present with pruritus and appears as “cracked porcelain” with irregular scaling and polygonal fissures.
Workup
A complete history (social, family, environmental, exposure history; past medical history, medications). Important factors to note:
Bathing habits: frequency and method; types of soaps/cleansers used
Emollient usage: frequency and method; types of emollients used
Dietary: fatty acid intake; fluid intake
Fabric contact: clothing, bedding (wool can exacerbate symptoms)
Common complaints: scaling, tightness, chapping; exacerbation of symptoms in winter
Conduct a focused physical examination, including thyroid and full skin exam
Can present as localized or generalized, commonly on extremities
Extremely dry skin presents with redness, cracking, scaling
Scratching may be evidenced by excoriations
Diagnostic Workup
For cases of acute onset and those associated with systemic symptoms, consider complete blood count (CBC), thyroid function tests, blood urea nitrogen (BUN) and creatinine, liver function tests, human immunodeficiency virus (HIV) testing, chest X-ray, erythrocyte sedimentation rate (ESR), immunoglobulin E (IgE), antinuclear antibody (ANA), and C-reactive protein (CRP)
If conservative therapy fails, consider age-appropriate malignancy screening
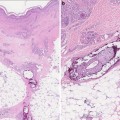
Histology
Biopsies are rarely indicated as dry skin can be easily diagnosed clinically. Histological findings include atrophy of the pilosebaceous follicles and eccrine sweat glands [16].
Treatment
Patients should apply petroleum or non-petroleum based hypoallergenic emollients to moist or wet skin daily, and should be advised to avoid excessive hand washing or showering which strip the skin of natural oils [4]. Neutral-pH products or liquid cleansers containing petrolatum should be used instead of harsh antibacterial soaps. For scaly patches without fissures, lactic acid containing moisturizers are indicated. To ensure adequate hydration, a cool mist humidifier may be used during dry winter months. The diet should include adequate water intake, appropriate for a CKD patient, and adequate intake of essential fatty acids. Cotton clothing and bedding should be used instead of wool and other irritating fabrics.
Drugs
Emollients aim to target the key abnormalities of xerosis, including inadequate water transport to the stratum corneum; poor water-binding; and barrier disturbances. Both classes of emollients, those comprising oil-in-water emulsions (light formulation) with 5 % urea and those comprising water-in-oil emulsions (rich formulation) with 10 % urea, applied twice daily over a 2-week period are effective in alleviating dryness and scaling [17, 18]. Table 6.1 includes a list of important emollient ingredients with specific roles in treatment of xerosis. Although a single emollient may not contain all of the listed ingredients, formulations combining ingredients which serve different purposes, such as humectants, physiological lipids, and natural moisturizing factors (NMF), are effective in treating xerosis [10]. A number of clinical studies have shown improvement in dryness with drugs containing urea, dexpanthenol, ammonium lactate, lactate, lactic acid, and/or pyrrolidone carboxylic acid as active substances (Table 6.2).




Table 6.1
Important ingredients and functions in emollients
Ingredient | Role |
|---|---|
Non-physiological lipids (petrolatum, mineral, vegetable oil) | Replaces lost natural skin lipids, improve barrier function |
Physiological lipids (ceramides, free fatty acids, cholesterol) | Repairs damaged intracellular lipid lamellae [19]; promotes epidermal differentiation through signaling (ceramides); increases lipid content of stratum corneum; improves barrier function |
Glycerol (humectant) | Treats symptoms not due to lipid depletion: restores normal aquaporin-3 function for skin hydration and elasticity [20] |
Natural moisturizing factors (urea, lactate, potassium, amino acids, PCA, sugars) | Restores epidermal ion gradient to attract and retain water in stratum corneum [21] |
Antipruritics (glycine, NGF inhibitors, opioid receptor agonists, chamomile extracts, corticosteroids, endocannabinoids) | Glycine alleviates itching and reduce scratching by blocking histamine release from mastocytes [22] |
Inhibit nerve growth by blocking NGF [23] | |
Corticosteroids relieve inflammation; may cause skin thinning [24] | |
Endocannabinoids improve itch and dryness [25] | |
Dexpanthenol |
Table 6.2
Clinical studies on the effect of moisturizers on dry skin
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
