© Springer Science+Business Media New York 2015
Julia R. Nunley and Edgar V. Lerma (eds.)Dermatological Manifestations of Kidney Disease10.1007/978-1-4939-2395-3_99. Calcinosis Cutis
(1)
Department of Dermatology, Massachusetts General Hospital, 345 Franklin St., Apt. 404, Cambridge, MA 02139, USA
(2)
Massachusetts General Hospital, Harvard Medical School, 50 Staniford Street, Boston, MA 02114, USA
Keywords
Calcinosis cutisCutaneous calcificationMetastatic calcificationIntroduction
Calcium is essential in many tissues, including the skin, where it regulates epidermal proliferation, differentiation, and adhesion. When local or systemic insults perturb the factors regulating calcium, they may result in insoluble calcium salt deposition in the skin and subcutaneous tissue, known as calcinosis cutis. The condition is classified into four subtypes based on the presumed mechanism of calcium deposition: dystrophic, metastatic, iatrogenic, and idiopathic. This chapter expands on metastatic calcification, the subtype of calcification most commonly seen in renal disease and includes only limited discussions of subtypes usually seen independent of renal disease or discussed elsewhere in this textbook.
Pathogenesis
Metastatic Calcification
Metastatic calcification is characterized by precipitation of calcium salts in normal skin and soft tissue owing to abnormalities in calcium and/or phosphate metabolism. Decreased phosphate clearance and impaired synthesis of 1,25-OH vitamin D both contribute to derangements in calcium and phosphate levels [1]. Renal failure impairs 1-alpha-hydroxylation of vitamin D, thereby limiting calcium absorption from the intestine. Low serum calcium levels stimulate compensatory secondary hyperparathyroidism, normalizing calcium levels and further increasing phosphate levels. When the solubility product of calcium and phosphate (55 mg2/dl2) is exceeded, cutaneous and subcutaneous calcification might result.In patients with chronic renal failure calcinosis cutis might manifest as calciphylaxis or benign nodular calcification.
Calciphylaxis is the most severe form of metastatic calcification, occurring in as many as 4.1 % of patients undergoing hemodialysis, according to one retrospective review of 242 hemodialysis patients [2]. The pathogenesis remains poorly understood but is likely multifactorial—time-averaged elevation of the calcium/phosphate product, a hypercoagulable state due to reduced protein C and S, hyperparathyroidism and skin trauma are all thought to be contributing factors. Multiple risk factors have been identified including female sex, obesity, diabetes, and the use of calcium-based phosphate binders.
Less common causes of metastatic calcification independent of renal disease include milk-alkali syndrome (excessive intake of calcium-containing foods) and hypervitaminosis D (prolonged intake of supratherapeutic doses of vitamin D).
Other Forms of Calcification
Dystrophic calcification is the most common type of calcinosis cutis. It is thought to be secondary to local insults in the absence of derangements in systemic calcium metabolism. The pathogenesis is unclear; however, one proposed mechanism implicates necrotic cell debris that is thought to serve as a nidus for ectopic calcification; further, alterations in collagen, elastin, and the subcutis are thought to promote calcification.
Iatrogenic calcification refers to deposition of calcium salts as a result of medical intervention, usually intravenous calcium chloride or calcium gluconate [3–5]. The etiology is thought to be both locally elevated tissue concentration of calcium, and tissue injury at the site of extravasated calcium.
Idiopathic calcification is the category reserved for cutaneous calcification seen in the absence of an underlying tissue damage or metabolic disorder. It comprises acne-induced, milia-like, tumoral, subepidermal calcified nodules, scrotal calcinosis.
Clinical Presentation
Soft tissue calcification commonly complicates chronic renal failure: estimates regarding its prevalence range from approximately 40 %, to as high as 80 % in one autopsy study of hemodialysis patients [6]. Please see Chap. 10 for details on clinical presentation and treatment of calciphylaxis.
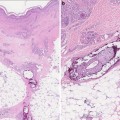
The most common type of cutaneous calcification seen in CKD is metastatic calcification.Benign nodular calcification, the most common subtype, is defined as cutaneous and subcutaneous tissue calcification in the absence of tissue necrosis. Lesions are typically painless, firm, papules, plaques or nodules that occur most commonly around joints and on the fingertips [7, 8]. Long-standing secondary hyperparathyroidism predisposes to this condition; the number and size of the calcium deposits are directly proportional to the degree of hyperphosphatemia. Similar findings are seen in tumoral calcinosis, an inherited or acquired abnormality of phosphate homeostasis independent of renal function [9].Although it is often seen in otherwise healthy individuals, it might also be triggered by the uremic mileu.
Dystrophic calcification in CKD is more commonly observed in patients with connective tissue diseases, especially CREST syndrome (calcinosis cutis, Raynaud phenomenon, esophageal dysfunction, sclerodactyly, and telangiectasia) and lupus panniculitis.However, it can also be seen in patients with comorbidities including pancreatic panniculitis, various inherited disorders such as Ehlers-Danlos, cutaneous neoplasms (pilomatricomas, pilar cysts), and infections (onchocerciasis, cysticercosis).Calcified lesions are usually localized to the area affected by the underlying condition.
Iatrogenic calcification occurs as a complication of a procedure, such as extravasation during intravenous administration of solutions containing calcium or phosphate or prolonged contact with calcium chloride electrode paste during electroencephalography [9]. Lesions develop at the site of the inciting event.
Though uncommon, idiopathic calcinosis can also be seen in patients with CKD.Subepidermal calcified nodules present as isolated hard 3–11 mm white-to-yellow papules over the head and extremities, usually in children. These might represent calcified adnexal structures according to one study [10]. Scrotal calcinosis, characterized by marble-like subcutaneous nodules varying in size and number, are thought to arise from epidermal or eccrine cysts. They are usually asymptomatic although minimal pruritus or a white chalky discharge may be noted.Milia-like calcinosis consists of tiny white pearly papules (“milia-like” lesions) on the dorsal surface of the hands and face; they are most commonly seen in patients with Down syndrome. Although there are usually no preexisting lesions, some appear to due to calcification of pre-existing syringomas.
Milia-like calcinosis characterized by tiny white pearly papules (“milia-like” lesions) on the dorsal surface of the hands and face, most commonly seen in the setting of Down syndrome. There are usually no preexisting lesions, although in some patients they appear to arise from calcification of precursor syringomas.
Laboratory Abnormalities
In metastatic calcification, theoretically, precipitation occurs when levels of calcium and phosphate exceed their solubility product, although one study found clinically elevated calcium or phosphate levels in only a fraction of patients with metastatic calcification [11].
Serum calcium and phosphate levels are within normal limits in dystrophic calcification and in idiopathic calcification (except for tumoral calcinosis).
Treatment
Drugs
Aluminum Hydroxide
Dosage: 1.8–2.4 g daily.
Mechanism of action: Aluminum hydroxide taken orally complexes with phosphate to form an insoluble precipitate that limits intestinal absorption of phosphate. The resulting decrease in phosphate levels is thought to hinder or even reverse the development of ectopic calcifications [6].
Effectiveness




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
