Fig. 4.1
SWO schematic drawing showing fungal invasion of the dorsal nail plate
Fig. 4.2
SWO dermoscopy shows that the superficial nail plate is affected
Epidemiology
Onychomycosis generally affects men more commonly than it affects women. Associated factors include diminished peripheral circulation, diabetes, trauma to the nail, and inadequate nail hygiene [10]. SWO is a rare type of onychomycosis that constitutes 1.5–7 % of all reported cases of fungal nail infections [11]. While SWO affects about 1–2 % of the general population, the incidence increases with age. Rate of prevalence is higher in the immunosuppressed, with 9.5 % of HIV-infected patients reportedly affected by SWO [7]. However, epidemiological characteristics may also vary according to the variant of SWO involved.
Clinical Features
There are two main subtypes of SWO: classical SWO and deep SWO (Figs. 4.3 and 4.4). In classical SWO, the superficial nail plate presents small white opaque friable patches with distinct borders. Scraping of the patches allows removal of the whitish surface material, exposing a transparent compact median nail plate. Sometimes, the patches may coalesce with time to involve the entire nail that becomes diffusely milky, white, and opaque [1, 3, 7]. One variant of classical SWO involves a route of infection that arises from below the proximal nail fold. This form of SWO, which may be difficult to distinguish from proximal subungual onychomycosis (PSO), most commonly affects children, who have thin nails, or immunosuppressed patients [1, 3]. In some cases, this variant presents with striate superficial bands, with affected white bands alternating with unaffected nail (Fig. 4.5). Deep invasion of the nail plate usually results from infection with non-dermatophytic molds, such as Fusarium and Aspergillus species, due to their eroding bodies which enable penetration of the nail plate barrier (Fig. 4.6) [4]. This deep variant is characterized by diffuse white and yellow-brown patches (Figs. 4.7 and 4.8). Nail plate discoloration may extend to the proximal nail fold, and the pigmentation can be visible through the cuticle [7]. Combination of SWO with another type of onychomycosis, such as distal and lateral subungual onychomycosis (DLSO) or proximal subungual onychomycosis (PSO), is not uncommon (Figs. 4.9 and 4.10) [1, 2].






Fig. 4.3
SWO classical type
Fig. 4.4
Deep SWO
Fig. 4.5
SWO with striated pattern
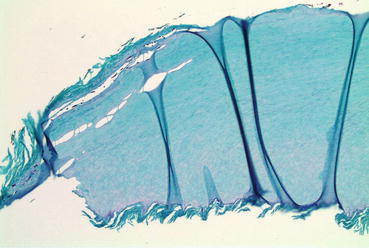
Fig. 4.6
Deep SWO: pathology shows fungal elements in the superficial and mid-nail plate
Fig. 4.7
SWO yellowish desquamating patch
Fig. 4.8
SWO: note the yellow-white discoloration and crumbling of the nail surface
Fig. 4.9
SWO and DLSO affecting the same nail
Fig. 4.10
SWO emerging from proximal nail fold and DLSO
Diagnostic Clues
It is important to conduct mycological studies, in order to appropriately diagnose and treat onychomycosis [10]. Diagnosing SWO may be performed using direct microscopy with 40 % potassium hydroxide (KOH) mounts, fungal cultures, and nail clippings with periodic acid-Schiff (PAS) staining for histologic analysis (Fig. 4.11) [7, 12]. In some cases of SWO, taking a clipping might be difficult, as the infection is often located in the central part of the nail plate without involvement of the distal nail. Scraping of the superficial nail plate is the best way to obtain samples for KOH and culture. Of note, potassium hydroxide microscopy and culture carry a relatively low negative predictive value (<60 %) and, therefore, warrant repeat testing in patients with possible SWO that initially test negative [12].