Key points
- •
Non-surgical, minimally invasive alternative to surgery.
- •
Injectable fillers commonly used for skin wrinkles, deep creases, depressed scars and regional volume enhancement of the face.
- •
Filler selection largely based on duration of enhancement and anatomic area of concern.
- •
Establish a conservative approach with gradual reshaping over time.
- •
Utilize appropriate injection technique with proper plane for filler deposition.
Patient selection
Over the last two decades, the concept of using injectable fillers for facial rejuvenation has become a well accepted standard in the practice of plastic surgery. The ideal patient for injectable filler use in the face is one who desires a non-surgical, minimally invasive approach for aesthetic soft tissue volumetric enhancement. The best candidates tend to be younger, middle-aged patients, as this population typically requires only mild to moderate change for early signs of aging. In those with more advanced aging changes requiring more extensive volumetric enhancement, surgical treatments options, such as facial implants or lifting, may be more beneficial. Even in this population of patients, injectable fillers can be used as a powerful adjunct in augmenting or complementing a surgical result.
Indications
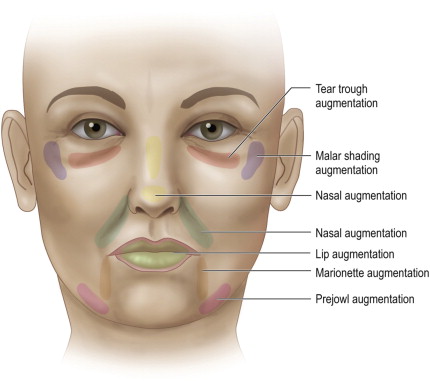
As the number of injectable fillers has steadily increased since their introduction decades ago, so has the array of indications for their use in the face ( Figure 7.1 ). For many years now, one of the most popular indications has been smoothing out unwanted facial wrinkles and creases. As we age, the collagen framework that normally provides support to the dermal skin layer gradually begins to loosen. Over time, this results in dermal thinning and focal reduction of soft tissue volume. Eventually this leads to formation of a fine wrinkle or crease within the skin. With further aging and gravitational pull, fine wrinkles and creases can deepen into what are essentially skin folds. Glabellar frown lines are a common example of this aging process. When injectable fillers are used to treat a skin wrinkle or crease, the intention is to replenish the dermal collagen that was lost as a result of the aging process. Hence the term dermal filler commonly used to describe this particular application. By volumetrically expanding, or plumping, the dermal layer, injectable fillers can help decrease or even eliminate wrinkle depth to restore a smooth skin surface.
Perhaps the most well-known example of a deepened skin crease is the nasolabial fold. This represents what happens when a naturally shallow crease in youth deepens considerably with the aging process. It should be pointed out that it is aesthetically acceptable to have a fine line between the cheek and upper lip. When this line begins to deepen and create an abnormal shadow, injectable fillers may be indicated. The goal of correction should be to restore a fine or shallow line rather than completely erase any perception of demarcation. In patients who have undergone prior facelift surgery, soft tissue volume enhancement of the nasolabial fold can be a powerful complementary procedure to further augment their results.
An extension of wrinkle treatment is injectable filler use for depressed scars. Although unrelated to the aging process, depressed scars also demonstrate marked thinning of the dermal collagen layer similar to what is seen in wrinkles and creases. Such scars are commonly seen in patients with a history of recurrent acne or prior traumatic injury that causes damage to the dermis. This results in focal loss of dermal collagen that leads to an unwanted depression along the skin with unwanted shadowing. In an analogous fashion for wrinkles or creases, injectable fillers are used to replace the lost collagen, which essentially raises the depressed scar and smoothes out the skin surface.
Another widely popular indication for injectable filler use in the face is regional volume deficiency. This refers to broader aesthetic subunits, or regions, of the face that are lacking in sufficient shape and contour. Unlike wrinkles or creases, this type of contour abnormality often results from volume deficiency below the dermal plane. Depending on the area, this can include deficiencies in subcutaneous fat, muscle and/or mucosa. In some cases this involves patients who are seeking to aesthetically enhance a certain area that is naturally deficient in volume. In others, injectable fillers are being used to rejuvenate or correct volume deficiencies that are more related to the aging process or iatrogenic causes.
A common example of regional volume deficiency is the tear trough/malar region. In younger patients who present with this type of volume deficiency, it usually reflects a congenital predisposition to hollowing below the lower eyelid. In the more aged population, this scenario is due to infraorbital fat pads that appear to herniate forward in combination with descent and flattening of the malar fat pad. The end result is disruption of the naturally youthful convexity that normally extends from the lower eyelid to the malar region. The clinical manifestation of this is an excessively tired look due to puffy lower eyelids and unmasking of the tear trough. Most patients complain of unwanted shadowing and hollowing involving this area that contributes to a prematurely aged appearance. Injectable fillers can be quite beneficial in this setting by volumetrically expanding the tear trough with or without augmentation of the malar eminence. This helps to restore an uninterrupted convexity by blending the lower eyelid and malar region resulting in a more rested look.
The perioral region is another area frequently treated with injectable fillers. This region, which includes the lips, marionette lines and prejowl sulcus, is considered the predominant aesthetic unit of the lower third of the face. Central to this region is the appearance of the lips, which includes the philtral columns. In today’s society, fuller shapely lips are synonymous with a more feminine and sensual appearance. Younger patients presenting for lip augmentation typically only require additional volume. This usually involves injection of the mucosal lip, vermilion border and philtral columns in combination to achieve an enhanced shape. This also includes increased definition of Cupid’s bow in the upper lip. In the more senescent population, several other factors must also be considered due to age-related submucosal atrophy. These patients demonstrate further degrees of volume deficiency giving the appearance of even more deflated lips. In addition, these changes are accompanied by formation of perioral vertical lip lines. Therefore, the senescent lip demands not only volume enhancement but also management of vertical lip lines to help restore a more youthful definition.
When assessing candidacy for lip augmentation, it is critical to evaluate the other components of the perioral region, such as the marionette lines and prejowl sulcus. Combined treatment of these areas is commonly indicated to achieve optimal lower face rejuvenation. Marionette lines refer to the soft tissue fold that develops at the lateral oral commissure. Often seen in conjunction with atrophic lip changes, these lines descend in a downward direction from the corner of the mouth. This often contributes to a sad and prematurely aged appearance. Injectable fillers work by effacing these lines, which helps give the appearance of elevating the corner of the mouth. In patients with hyperdynamic movement of the underlying depressor anguli oris (DAO) muscle, concurrent use of botulinum toxin can further enhance the results of an injectable filler.
With aging, sagging skin and underlying bone resorption contribute to formation of the jowl. This is an abnormal soft tissue contour that disrupts the normally youthful jawline. As a result, an abnormal oblique shadow is created between the jowl and chin corresponding to the prejowl sulcus. In an attempt to eliminate this shadow facelift surgery and chin implants are frequently employed to suspend the jowl and fill in the soft tissue void, respectively. As a non-surgical alternative, injectable fillers can be used quite effectively to volumetrically expand the prejowl sulcus. By elevating this soft tissue depression a smoother, more youthful transition can be restored from the chin to the posterior jawline.
A recent and growing indication for injectable filler use is an undesirable nasal appearance. In patients who would otherwise undergo augmentation rhinoplasty, perinasal injectable fillers can be used as an alternative to elevate or project certain areas of the nose, such as the radix, bridge and tip. This method has gained increasing popularity and is often referred to as injection rhinoplasty. Injectable fillers are also quite useful in patients who have already undergone rhinoplasty and note persistent postoperative contour irregularities or depressions. Instead of undergoing a complex and risky secondary rhinoplasty procedure, injectable fillers can be used as a minimally invasive option to achieve the anticipated result.
Fillers may also be used in cases where an alloplastic implant would have otherwise been placed. The malar regions, perinasal skeleton, mandibular angles and chin are all amendable to volume augmentation by fillers. Fillers may be used as a prelude to placement of permanent implants or on a periodic basis in patients desiring temporary improvement. Augmentation of the facial skeleton by fillers is one of the most subtle, but powerful non-surgical treatments that can be offered and may yield at times dramatic improvement in soft tissue drape.
Injectable filler selection
Over the last decade there has been a dramatic increase in the number of fillers available for volumetric enhancement of the face. This reflects the fact that the ideal injectable filler has yet to be introduced. The ideal filler would be a material that is biocompatible, non-allergenic, easy to administer, long lasting, non-migratory, economical, and predictable in terms of results. Most fillers currently available possess at least several of these desired properties. A majority are bioengineered materials that can be used interchangeably for many different applications. With such a vast number of fillers to choose from, a helpful approach for many surgeons is to categorize them based on duration of enhancement – temporary, long lasting and permanent. Individual selection can then be further tailored depending on the anatomic area of concern and what works best in your hands.
Temporary injectable fillers
Temporary injectable fillers are products that provide clinical enhancement on average between 6–9 months in duration. Hyaluronic acid (HA) based materials comprise a majority of the temporary fillers currently used. These fillers are predominantly synthetic products derived from non-animal stabilized hyaluronic acid (NASHA). Thus, they do not require allergy skin testing prior to injection. Hyaluronic acid products are ideally suited for use as injectable fillers because HA is natively present in the extracellular matrix of the human body. Hyaluronic acid is a linear polysaccharide with hydrophilic properties. With a high affinity for binding water molecules, HA plays a key role in hydrating the skin. This results in natural plumping and cushioning of the soft tissue layer. This effect is precisely why injectable HA can be used quite successfully in volume enhancement of the skin.
The primary difference between individual synthetic HA fillers available today is related to the various degree of cross-linking within each product. Chemical cross-linking alters the solubility of HA to create a more viscous, water insoluble gel form. This translates into a more stabilized product that can be properly stored as well as readily injected through a syringe. Higher degrees of cross-linking result in increased viscosity, which can influence inject technique and use for the various fillers. For example, less viscous gels allow for smoother injection and, thus, are better suited for superficial dermal injection. Products containing a higher viscosity gel are less forgiving and more prone to clumping. Therefore, these products should be injected along a mid to deep dermal plane to avoid superficial contour irregularities. Following placement, the HA undergoes gradual digestion with eventual clinical disappearance of the aesthetic effects by six to nine months. In most patients this duration of enhancement and need for repeat treatment is acceptable given the versatility and safety profile of HA fillers. In others, HA is considered more of a prelude to what a longer lasting or permanent filler may provide them in the future.
Prior to the introduction of HA based products, human derived collagen was considered the first choice in temporary filler use. Today, HA based products have largely supplanted these products. This is predominantly due to the fact that collagen products simply do not provide an adequate duration of enhancement. Clinical experience has demonstrated that collagen lasts only a number of weeks or several months at best. This would necessitate repeat treatment too frequently for most patients seeking injectable filler augmentation. One of the only remaining advantages of collagen use is for correction of very superficial fine lines, such as vertical lip lines. In this instance, collagen can be placed within the upper dermis to efface or smooth out individual lines. Because of its low viscosity, collagen can augment these fine lines with less risk of visibility or palpability compared with other fillers, such as hyaluronic acid.
Long lasting injectable fillers
Long lasting injectable fillers provide volume enhancement on average between 12 months and several years in duration. These fillers are largely composed of polymer microspheres suspended in a resorbable solution that slowly degrade over time. One of the most widely used fillers consists of 30% calcium hydroxylapatite microspheres (25–45 µm) suspended in an aqueous carrier gel. Like HA based products, calcium hydroxylapatite is relatively inert, very safe and requires no skin testing prior to injection. In comparison to HA based fillers, however, calcium hydroxylapatite is not recommended for treatment of more superficial wrinkles and creases. It is also not suggested for use in lip augmentation. The carrier gel typically absorbs soon after injection, leading to some degree of calcium hydroxylapatite precipitation. When injected superficially or into the lip, clumping can manifest as visible and palpable white nodules. It is worth noting that these nodules are not the same as granuloma formation. When placed in the mid to deep dermis or subcutaneous tissue space, there is ample soft tissue coverage to minimize visibility of the opaque filler. For this reason, calcium hydroxylapatite is more commonly used to augment moderate to deep creases and folds as well as regional volume deficiency. Around nine months after injection, calcium hydroxylapatite begins to undergo gradual enzymatic digestion with full disappearance of the aesthetic effect between twelve and eighteen months following placement.
Another popular long lasting filler is composed of polylactic acid microspheres (1–63 µm). Polylactic acid is a biosynthetic material that has been used safely for decades in the form of absorbable sutures, surgical plates and screws. With minimal antigenicity, no skin testing is required prior to injection. The product is packaged as a freeze-dried powder that is reconstituted using sterile water to produce a suspension of polylactic acid microspheres. Originally intended for treatment of human immunodeficiency virus drug-induced lipoatrophy, polylactic acid fillers are now considered to have a similar profile to calcium hydroxylapatite in terms of use. They are injected in the deep dermis or subcutaneous space to restore fullness to the face and reduce appearance of moderately deep wrinkles and folds. Once placed, the filler stimulates an inflammatory response from the body as it is metabolized to carbon dioxide and water. After several weeks, collagen deposition by the body begins to replace the volume occupied by the filler. Because this replacement process does not necessarily occur in a one to one volume ratio, three to five treatment sessions are required over a twelve to eighteen month period to gradually reach the desired level of augmentation. Such a lengthy period of time has been one of the biggest deterrents from more widespread acceptance of polylactic acid filler use.
Permanent injectable fillers
Permanent injectable fillers refer to products that are non-degradable and, thus, provide a durable aesthetic enhancement after placement.
Clinical experience has shown that PMMA fillers work best when injected in the deep dermis or subcutaneous layer so as to avoid unwanted ridging or papules in the skin. With proper level of placement, there is minimal inflammatory response elicited. The individual PMMA microspheres are eventually encapsulated by the patient’s own collagen as the bovine collagen disappears completely. The end result is a layer of biologically stabilized PMMA that resists migration and provides enduring soft tissue volume enhancement.
Procedural technique
Pre-procedure preparation
An essential key to success with injectable fillers is establishing a conservative approach with their use. This often translates into avoiding overcorrection. This is particularly important for the inexperienced surgeon using longer lasting and permanent fillers. Unfortunately, injectable filler use has been mischaracterized in the past as being a single session enhancement procedure. Instead, patients should be prepared by emphasizing their use as a gradual reshaping process that extends beyond the first treatment session. Patients should be counseled that the first treatment is intended to achieve a notable improvement in the area of concern. For optimal results, however, a follow-up appointment is routinely scheduled several weeks later for further augmentation and refinement.
Pre-procedure preparation for all injectable fillers also includes a detailed consultation to establish realistic patient expectations for the chosen product and planned area of treatment. Obtaining a medical history will help ensure absence of known hypersensitivity or allergic response to the material being placed. Other contraindications, such as pregnancy, lactation and a history of keloid or hypertrophic scar in cases of long lasting or permanent filler placement, should also be ruled out. Skin testing is recommended several weeks in advance of planned placement of any product containing bovine collagen.
Starting 10–14 days prior to treatment, patients should be restricted from using medications that would predispose to excess bleeding and swelling. Use of homeopathic supplements, such as arnica, before and after treatment has also proven successful in helping to minimize bleeding and swelling. Photodocumentation using adequate lighting and standard views is recommended to more accurately assess treatment outcomes. Written informed consent is also a prerequisite for injectable filler use.
Aesthetic analysis and determination of the volume deficient areas is accomplished with a thorough physical examination. This should also include notation of any pre-existing asymmetries, contour irregularities, and skin blemishes that may alter the proposed treatment outcome. Some injectable fillers require a preparatory lead-time before actual use. For instance, polylactic acid fillers are packaged in a powdered form and require reconstitution with sterile water prior to injection. It is recommended this be done 2–24 h prior to use to ensure complete hydration of the product. Others, such as PMMA fillers require storage in a refrigerator and, therefore, need to be thawed for 20–30 min prior to use.
Assessment of the required level of anesthesia is another important consideration prior to injection. It should be emphasized that a more comfortable patient will be less prone to procedure-related hypertension and, hence, ecchymosis and swelling. The simplest form of anesthesia involves use of a cold compress applied directly to the planned site of injection immediately prior to and after treatment. This is mostly commonly used when treating isolated wrinkles and creases. Another popular method is to apply a topical anesthetic to the skin 45–60 min prior to treatment. This should be done only after thoroughly cleansing the skin surface of all makeup and oil. For perioral injections, a cotton tip applicator can be used to swab the upper and lower labial sulcus. Due to a higher mucosal absorption rate, this method of anesthesia requires only a few minutes prior to filler placement.
In cases where topical anesthesia is thought to be insufficient, local or regional nerve blocks can be used for added patient comfort. After applying the topical anesthetic, 1–2% lidocaine with 1 : 100,000 epinephrine buffered with sodium bicarbonate is infiltrated in strategic sites depending on the area being treated. Careful attention must be paid to avoid excess infiltration as this may distort soft tissue contour and decrease accuracy of filler placement. For the tear trough or nasolabial fold, an infraorbital nerve block may be used to anesthetize the midface region. This is done by infiltrating approximately 0.25 mL at the exit site of the infraorbital nerve (V2) via transcutaneous or sublabial delivery. For lip augmentation, a regional block of the upper and lower lip can be quite effective. This involves distribution of approximately 0.5 mL across 4–5 sites along the upper or lower gingival sulcus. If more widespread perioral anesthesia is indicated for marionette lines and/or the prejowl sulcus, a mental nerve block may be performed. This is done by infiltrating approximately 0.25 mL at the exit site of the mental nerve (V3), which provides adequate anesthesia for augmentation of the lower lip and chin.
Related posts:
 Third generation polymethylmethacrylate (PMMA) aesthetic soft tissue fillers for the correction of nasolabial folds and other applications
Third generation polymethylmethacrylate (PMMA) aesthetic soft tissue fillers for the correction of nasolabial folds and other applications
 Injectable silicone: current role
Injectable silicone: current role
 Poly -l-lactic acid (Sculptra®)
Poly -l-lactic acid (Sculptra®)
 Avoidance and treatment of complications after dermal filler injections
Avoidance and treatment of complications after dermal filler injections
 Possible causes and treatment options of dermal filler granulomas
Possible causes and treatment options of dermal filler granulomas
 Shaping the future: new outcomes in Europe
Shaping the future: new outcomes in Europe
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


