Vertical Mammaplasty for Breast Reduction and Mastopexy
Albert De Mey
Diane Franck
Christophe Zirak
Few operations can be considered entirely new, as one always borrows from the past to describe a surgical technique. After the description of Dartigues in 1925 (1) and Arie in 1957 (2), Lassus published a vertical scar mammaplasty in 1970 (3). The vertical mammaplasty that we will describe is derived from the technique of Lassus (4) and modified by Lejour (5) to be applicable for small breasts, as well as for large ones. The operative technique of vertical scar mammaplasty described in this chapter represents evolution based on an experience of more than 20 years of performing this technique.
Initial results obtained using the technique of Lejour (6,7) have been encouraging not only concerning the reduction of scar, but also for the achievement of a long-lasting, good-looking breast (see Fig. 88.10). The Lejour technique has been used in our department as the only technique for breast reduction since 1990. However, at the university hospital, a high rate of complications was observed when the technique was performed by multiple operators, often residents in training. This is probably due to the fact that the technique as described and performed by Lejour was based on experience in hundreds of these procedures associated with an uncommon skill. This made the outcome of that particular technique not always predictable in other hands.
In order to reduce the learning curve and make it easily applicable and teachable in a plastic surgery training center, some modifications were adopted that proved to be effective in reducing the risks of complications or unsatisfactory results (8,9) and also to be applicable even in large breasts (10).
The modified technique remains based on a superiorly based areolar pedicle with central glandular resection. Extensive wide lower skin undermining is avoided, as well as liposuction of the breast. The shape of the breast is created by suturing the gland and does not rely on the skin to maintain its form. In the majority of cases, no scar is needed in the submammary fold.
Principles
The goals of a breast reduction are correcting the volume, improving durability of the shape and symmetry, and preserving nipple sensitivity with minimal scarring.
Volume reduction and correction of the shape can be obtained by different techniques. However, long-term results remain a concern because too often the result of surgery deteriorates with time, especially in large breasts. A high projected and narrowly based breast must be obtained and maintained. In the vertical scar mammaplasty, the reshaping is based on the suture of the glandular pillars in the medial inferior quadrant of the breast.
Scars are unavoidable but should be minimal. This, of course, must not be at the expense of the quality of breast shape. The periareolar scar is mandatory, as the nipple/areola has to be repositioned. Periareolar techniques have been described but are only applicable to small reductions and often result in a flat breast with stretched areola and irregular scars. The vertical scar allows an adequate reduction of the skin brassiere over the reduced breast volume in most cases and is the scar that fades best with time. In our technique, the horizontal submammary scar can be avoided in the majority of cases except for the reduction of more than 1,000 g per breast and inelastic skin (10). However, it can be limited in length and always well hidden in the breast fold.
Drawings
The preoperative drawings are done the day before surgery, according to the description of Lejour (5), on a standing patient.
The future nipple site is positioned on a line joining the suprasternal notch with the nipple slightly lower than the inframammary sulcus as projected to the face of the breast by the index finger (Fig. 88.1). The areolar circumference is then defined by marking the upper pole on the line drawn from the nipple to the sternal notch 2 cm above the nipple site. This distance between the sternal notch and the areolar site is 18 to 22 cm. The internal limit of the areola is positioned at 9 to 10 cm from the midline, according to the width of the chest, and the external limit 7 to 8 cm externally of this point on a horizontal line drawn 3 to 4 cm below the upper marking. These three points are joined and mark the superior areolar circumference.
The submammary fold is marked, as well as the vertical axis of the breast.
The lateral markings are made by pushing the breast laterally and medially with an upward rotation movement, in continuity with the vertical axis drawn below the breast (Fig. 88.2A, B).
The lower limits of the areola are then delineated by drawing a slightly curved line between the previous areolar points and the vertical lines (Fig. 88.3). The total circumference of the areola must measure between 14 and 16 cm to match the 4.2-cm areola template.
The same markings are made on the opposite breast. To check the symmetry of the drawings, the breasts can be gently pushed together toward the midline, making the medial markings touch.
Surgical Technique
Under general anesthesia, the patient is positioned in a semisitting position, with the hands under the buttocks. The base of the breast is constricted with an autofixed band Mammostat, and the periareolar area is deepithelialized. Two points are
then marked on each vertical line 7 to 8 cm below the lower areolar point in order to determine the height of the remaining glandular pillars (Fig. 88.4).
then marked on each vertical line 7 to 8 cm below the lower areolar point in order to determine the height of the remaining glandular pillars (Fig. 88.4).
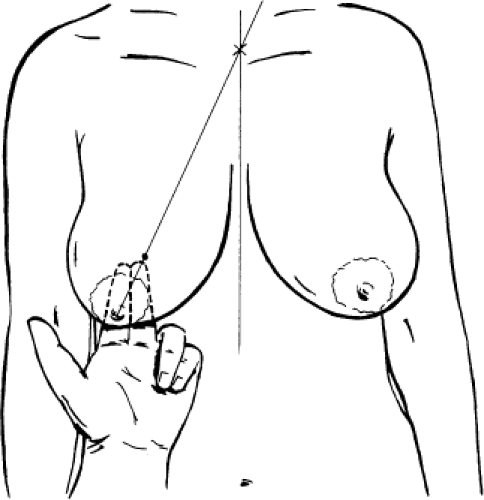 Figure 88.1. Marking of the future nipple site. |
A skin hook is placed at this point and another at the lowest part of the drawings near the submammary fold. This makes it possible to undermine the lower part of the breast subdermally, leaving not too much adipose/glandular tissue attached to the dermis down to the submammary sulcus. This dissection is performed both medially and laterally in the inferior quadrants of the breast (Fig. 88.5).
Related posts:
 Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy
Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy
 Breast Implants: Materials and Manufacturing Past, Present, and Future
Breast Implants: Materials and Manufacturing Past, Present, and Future
 Reconstruction of the Irradiated Breast
Reconstruction of the Irradiated Breast
 Perforator Flaps in Breast Reconstruction
Perforator Flaps in Breast Reconstruction
 Lipomodeling of the Reconstructed Breast
Lipomodeling of the Reconstructed Breast
 The Periareolar Approach to Augmentation Mammaplasty
The Periareolar Approach to Augmentation Mammaplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


