Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Michael D. Sgroi
Jason T. Lee
DEFINITIONS
Peripheral arterial disease (PAD) affects 8 to 12 million people worldwide.
Up to 40% of these patients suffer from poor quality of life due to impaired walking ability, nonhealing wounds, and need for amputation.
Risk factors include male gender, age, hypertension, diabetes, hyperlipidemia, renovascular disease, and smoking.
Sixty to ninety percent of patients with peripheral arterial disease also have coronary artery disease, and up to 25% have carotid artery stenosis.1
The overall 5-year mortality rate among all patients with PAD is 15% to 30%, and the risk of nonfatal myocardial infarction or stroke is 20% at 5 years.2
Patients with critical limb ischemia have an annual cardiovascular mortality of 25% and an annual amputation rate of 25%.3
ANATOMY
Femoral artery usually lies one-third the distance from the pubic tubercle and two-thirds from the anterior superior iliac spine.
Lateral dissection at the femoral artery should be minimized so not to disrupt the femoral nerve.
Medial dissection at the femoral artery should be minimized so not to damage the femoral vein.
Exposure of the common femoral artery should include the distal external iliac artery under the inguinal ligament.
Care should be taken to identify all distal branches (superficial femoral artery (SFA) and profunda femoris).
Anterior tibial artery runs in the anterior compartment of the leg.
Anterior tibial artery is between the anterior tibialis and extensor digitorum longus muscles.
Anterior tibial artery becomes the dorsalis pedis when it crosses the ankle joint.
Dorsalis pedis can be palpated just lateral to extensor hallucis longus on the dorsum of the foot.
Posterior tibial artery carries blood through the posterior compartment of the leg and plantar surface of the foot.
Posterior tibial artery branches into the medial and lateral plantar arteries in the foot.
Posterior tibial artery can be palpated midway between the medial malleolus and the Achilles tendon.
PATIENT HISTORY AND PHYSICAL FINDINGS
Ischemic claudication (ie, arterial perfusion inadequate to meet the demands of the muscle) leads to cramping, aching pain.
Claudication will usually occur one vascular level below the stenosis or occlusion.
Ischemic rest pain (ie, chronic ischemic neuropathy that is positional) is often described as diffuse aching or burning while legs are up in recumbent position, which is improved after legs have been put in the dependent position.
Vascular and neurogenic claudication must first be differentiated.
Infrapopliteal disease is most often going to lead to ankle and foot disease.
Patients with tibial disease are more likely to experience rest pain or have nonhealing wounds rather than claudication symptoms.
Ulcers to the medial side of the ankle are more likely due to venous disease.
Ulcers to the lateral food and ankle are more likely to be due to arterial disease.
IMAGING AND OTHER DIAGNOSTIC STUDIES
An ankle-brachial index (ABI) may be obtained by dividing the systolic blood pressure of the lower leg/ankle by the systolic blood pressure of the upper arm (brachial artery) (FIG 1).
An ABI ≤ 0.9 is considered abnormal.
ABIs will most commonly be indeterminate because the tibial vessels become noncompressible and waveforms will be monophasic.
Toe-brachial pressures (TBIs) will be more diagnostic in patients with tibial disease.
A TBI < 0.4 will indicate a wound is unlikely to heal without intervention.
Arteriography should be performed to evaluate the tibial vessels prior to any distal lower extremity or foot reconstruction.
Patients with diabetes and end-stage renal disease most frequently are affected by small vessel disease, including tibial vessels and the microvascular circulation.
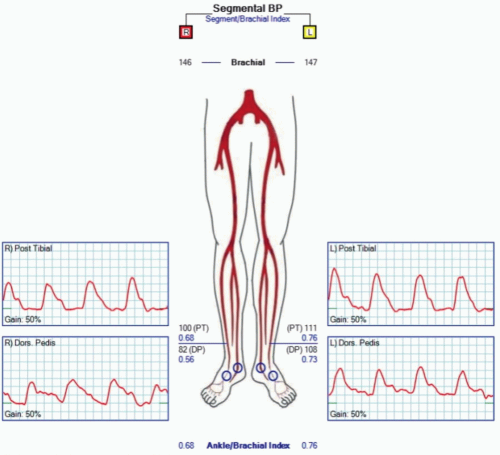 FIG 1 • Example of an abnormal ankle-brachial index study. |
SURGICAL MANAGEMENT
A patient must first have an appropriate inflow and outflow vessel identified for reconstruction.
Autologous vein has superior rates of patency compared to prosthetic grafts.
Vein mapping should be performed preoperatively, assuring at least a 3-mm conduit.
Shorter bypass grafts have better patency.
The most distal patent native vessel should be used as the proximal origin of the bypass graft.
For example, if the patient has a patent popliteal artery, this should be chosen over a femoral artery.
Primary patency (the patency of a graft without any adjunctive therapies to keep it open), secondary patency (the patency rate once the graft has been completely abandoned and no further interventions are performed to keep it open), and limb salvage rates are 56.8%, 62.7%, and 78.2%, respectively, at 5 years for pedal revascularizations.
TECHNIQUES
▪ Femoropopliteal Bypass
Identification of the femoral artery should be within the femoral triangle.
Femoral triangle consists of the inguinal ligament superiorly, sartorius muscle laterally, and the adductor magnus medially.
The floor of the femoral triangle consists of the iliacus, psoas major, pectineus, and adductor magnus.
The femoral artery is a continuation of the external iliac artery below the inguinal ligament.
Common femoral artery divides into the profunda femoral artery and the superficial femoral artery.
The profunda femoral gives branches to the thigh and collaterals to the lower extremity.
The superficial femoral artery is a continuation of the common femoral artery and progresses to the popliteal artery.
Longitudinal incision is made over the pulse in the groin, which is usually located below the inguinal ligament approximately one-third lateral to the pubic tubercle (TECH FIG 1A).
Dissection is taken down through the fascia lata, keeping medial to the sartorius muscle (TECH FIG 1B).
The superior limit of the groin dissection is the inguinal ligament. Retraction of the ligament exposes the external iliac artery.
The inguinal ligament can be further retracted by laterally dissecting along the ligament releasing all attachments.
Once under the ligament, the inferior epigastric vein should be identified and ligated.
Profunda femoral artery divides into the adductor fascia. Dissection along the anterior surface can be performed, identifying each of its branches (TECH FIG 1C,D).
Care should be taken not to dissect into the deep lateral circumflex femoral vein, which lies across the proximal profunda.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Achilles Tendon Reconstruction
Achilles Tendon Reconstruction
 Soft Tissue Coverage of Lower Leg—Soleus Flap
Soft Tissue Coverage of Lower Leg—Soleus Flap
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


