Key Words
urticaria, angioedema, pregnancy dermatoses, dermographism, cholinergic urticaria, serum sickness, mastocytosis, anaphylaxis, acquired angioedema, C1 INH deficiency syndrome
Urticaria, also referred to as hives or wheals, is a common and distinctive cutaneous reaction pattern. Hives may occur at any age; up to 20% of the population will have at least one episode. Hives may be more common in atopic patients. Urticaria is classified as acute or chronic. The majority of cases are acute, lasting from hours to a few weeks. Angioedema frequently occurs with acute urticaria, which is more common in children and young adults. Chronic urticaria (CU; arbitrarily defined as episodes of urticaria lasting more than 6 weeks) is more common in middle-aged women.
Because most individuals can diagnose urticaria and realize that it is a self-limited condition, they do not seek medical attention.
The cause of acute urticaria is determined in many cases, but the cause of CU is determined in only 5% to 20% of cases. Patients with CU present a frustrating problem in diagnosis and management. History taking is crucial but tedious, and treatment is usually supportive rather than curative.
These patients are often subjected to detailed and expensive medical evaluations that usually prove unrewarding. Studies demonstrate the value of a complete history and physical examination followed by the judicious use of laboratory studies in evaluating the results of the history and physical examination.
Clinical Aspects
Definition.
A hive or wheal is a circumscribed, erythematous or white, nonpitting, edematous, usually pruritic plaque that changes in size and shape by peripheral extension or regression during the few hours or days that the individual lesion exists. The edematous central area (wheal) can be pale in comparison to the erythematous surrounding area (flare).
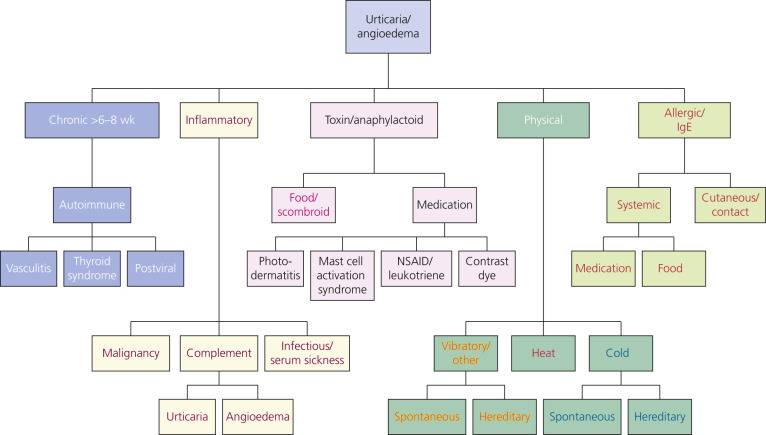
The evolution of urticaria is a dynamic process. New lesions evolve as old ones resolve. Hives result from localized capillary vasodilation, followed by transudation of protein-rich fluid into the surrounding tissue; they resolve when the fluid is slowly reabsorbed. The edema in urticaria is found in the superficial dermis. Lesions of angioedema are less well demarcated. The edema in angioedema is found in the deep dermis or subcutaneous/submucosal locations. The differential diagnosis of hives is found in Box 6.1 and Fig. 6.1 .
Bullous pemphigoid (urticarial stage)
Dermatitis herpetiformis
Drug eruptions
Erythema marginatum
Erythema multiforme
Papular urticaria
Pruritic urticarial papules and plaques of pregnancy
Still disease
Urticaria pigmentosa
Urticarial vasculitis
Clinical Presentation.
Lesions vary in size from the 2- to 4-mm edematous papules of cholinergic urticaria to giant hives, a single lesion of which may cover an extremity. They may be round or oval; when confluent, they become polycyclic ( Figs. 6.2 to 6.9 ![]() ). A portion of the border either may not form or may be reabsorbed, giving the appearance of incomplete rings (see Fig. 6.4 ). Hives may be uniformly red or white, or the edematous border may be red and the remainder of the surface white. This variation in color is usually present in superficial hives; thicker plaques have a uniform color (see Figs. 6.2 to 6.7 ).
). A portion of the border either may not form or may be reabsorbed, giving the appearance of incomplete rings (see Fig. 6.4 ). Hives may be uniformly red or white, or the edematous border may be red and the remainder of the surface white. This variation in color is usually present in superficial hives; thicker plaques have a uniform color (see Figs. 6.2 to 6.7 ).



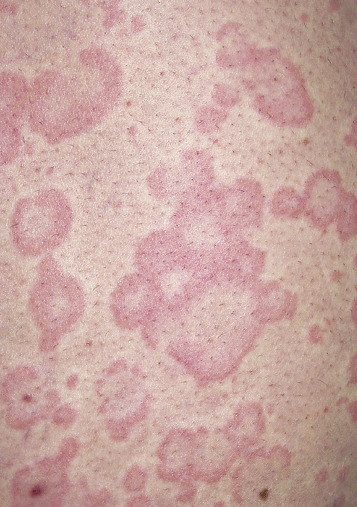




Hives may be surrounded by a clear or red halo. Thicker plaques that result from massive transudation of fluid into the dermis and subcutaneous tissue are referred to as angioedema. These thick, firm plaques, like typical hives, may occur on any skin surface, but typically involve the lips, larynx (causing hoarseness or a sore throat), and mucosa of the gastrointestinal (GI) tract (causing abdominal pain) (see Figs. 6.8 and 6.9 ). Bullae or purpura may appear in areas of intense swelling. Purpura and scaling may result as urticaria clear. Hives usually have a haphazard distribution, but those elicited by physical stimuli have characteristic features and distribution.
Symptoms.
Hives itch. The intensity varies, and some patients with a widespread eruption may experience little itching. Pruritus is milder in deep hives (angioedema) because the edema occurs in areas where there are fewer sensory nerve endings than there are near the surface of the skin.
Clinical Classification of Urticaria/Angioedema.
The CU subtypes are found in Box 6.2 .
Chronic Spontaneous Urticaria (CSU)
Spontaneous appearance of wheals, angioedema or both for >6 weeks due to known *
* For example, autoreactivity, i.e., the presence of mast cell–activating autoantibodies.
or unknown causes.Inducible Urticaria
Symptomatic dermographism †
† Also called urticaria factitia or dermographic urticaria.
Cold urticaria ‡
‡ Also called cold contact urticaria.
Delayed pressure urticaria §
§ Also called pressure urticaria.
Solar urticaria
Heat urticaria ¶
¶ Also called heat contact urticaria.
Vibratory angioedema
Cholinergic urticaria
Contact urticaria
Aquagenic urticaria
Urticaria can be provoked by immunologic and nonimmunologic mechanisms, as well as physical stimuli, skin contact, or small vessel vasculitis. Physical and ordinary urticarias may coexist. Angioedema occurs with or without urticaria. Angioedema without urticaria may indicate a C1 esterase inhibitor deficiency. The duration of hives is also an important diagnostic feature ( Table 6.1 ).
| Type of Urticaria | Duration |
|---|---|
| Ordinary and delayed pressure | 4–36 hours |
| Physical (except delayed pressure) | 30 min–2 hours |
| Contact (may have a delayed phase) | 1–2 hours |
| Urticarial vasculitis | 1–7 days |
Pathophysiology
Histamine
Histamine is the most important mediator of urticaria. Histamine is produced and stored in mast cells. There are several mechanisms for histamine release via mast cell surface receptors. A variety of immunologic, nonimmunologic, physical, and chemical stimuli may be responsible for the degranulation of mast cell granules and the release of histamine into the surrounding tissue and circulation. About one third of patients with CU have circulating functional histamine-releasing immunoglobulin G (IgG) autoantibodies that bind to the high-affinity IgE receptor (Fc epsilon RI). Release of mast cell mediators can cause inflammation and accumulation and activation of other cells, including eosinophils, neutrophils, and possibly basophils. Histamine causes endothelial cell contraction, which allows vascular fluid to leak between the cells through the vessel wall, contributing to tissue edema and wheal formation.
When injected into skin, histamine produces the “triple response” of Lewis, the features of which are local erythema (vasodilation), the flare characterized by erythema beyond the border of the local erythema, and a wheal produced from leakage of fluid from the postcapillary venule. Histamine induces vascular changes by a number of mechanisms ( Fig. 6.10 ). Blood vessels contain two (and possibly more) receptors for histamine. The two most studied are designated H 1 and H 2 .
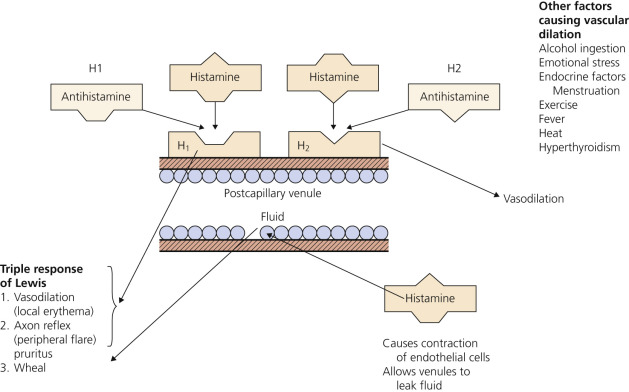
H 1 Receptors.
H 1 receptors, when stimulated by histamine, cause an axon reflex, vasodilation, and pruritus. Acting through H 1 receptors, histamine causes smooth muscle contraction in the respiratory and GI tracts and pruritus and sneezing by sensory nerve stimulation. H 1 receptors are blocked by the vast majority of clinically available antihistamines called H 1 antagonists (e.g., chlorpheniramine), which occupy the receptor site and prevent attachment of histamine.
H 2 Receptors.
When H 2 receptors are stimulated, vasodilation occurs. H 2 receptors are also present on the mast cell membrane surface and, when stimulated, further inhibit the production of histamine. Activation of H 2 receptors alone increases gastric acid secretion. Cimetidine, ranitidine, and famotidine are H 2 -blocking agents (antihistamines). H 2 receptors are present at other sites. Activation of both H 1 and H 2 receptors causes hypotension, tachycardia, flushing, and headache. The H 2 -blocking agents are used most often to suppress gastric acid secretion. They are used occasionally, usually in combination with an H 1 -blocking agent, to treat urticaria.
Initial Evaluation of All Patients With Urticaria
- 1.
Determine by skin examination that the patient actually has urticaria and not bites.
- 2.
Rule out the presence of physical urticaria to avoid an unnecessarily lengthy evaluation. Stroking the arm with the wood end of a cotton-tipped applicator will test for dermographism.
- 3.
Determine whether hives are acute or chronic. The difference in duration has been arbitrarily set at 6 weeks. Acute urticaria involves episodes of urticaria persisting less than 6 weeks. Chronic urticaria consists of recurrent episodes of widespread urticaria present for longer than 6 weeks.
- 4.
Review the known causes of urticaria listed in Box 6.3 (Etiologic Classification of Urticaria). Knowledge of the etiologic factors helps to direct the history and physical examination.
Box 6.3
From Geha R, Buckley CE, Greenberger P, et al. Aspartame is no more likely than placebo to cause urticaria/angioedema: results of a multicenter, randomized, double-blind, placebo-controlled, crossover study. J Allergy Clin Immunol 1993;92:513–20.
Etiologic Classification of Urticaria
Foods
Fish, shellfish, nuts, eggs, chocolate, strawberries, tomatoes, pork, cow’s milk, cheese, wheat, yeast
Food Additives
Salicylates, dyes such as tartrazine, benzoates, penicillin, aspartame (NutraSweet), *
* Probably does not cause hives.
sulfites
Drugs
Penicillin, aspirin, sulfonamides, and drugs that cause a nonimmunologic release of histamine (e.g., morphine, codeine, polymyxin, dextran, curare, quinine)
Infections
Chronic bacterial infections (e.g., sinus, dental, chest, gallbladder, urinary tract), Campylobacter enteritis, fungal infections (e.g., dermatophytosis, candidiasis), viral infections (e.g., hepatitis B prodromal reaction, infectious mononucleosis, coxsackie), protozoal and helminth infections (e.g., intestinal worms, malaria)
Inhalants
Pollens, mold spores, animal dander, house dust, aerosols, volatile chemicals
Internal Disease
Serum sickness, systemic lupus erythematosus, hyperthyroidism, autoimmune thyroid disease, carcinomas, lymphomas, juvenile rheumatoid arthritis (Still disease), leukocytoclastic vasculitis, polycythemia vera (acne urticaria: urticarial papule surmounted by a vesicle), rheumatic fever, some blood transfusion reactions
Physical Stimuli (Physical Urticarias)
Dermographism, pressure urticaria, cholinergic urticaria, exercise-induced anaphylactic syndrome, solar urticaria, cold urticaria, heat urticaria, vibratory urticaria, water (aquagenic) urticaria
Nonimmunologic Contact Urticaria
Plants (e.g., nettles), animals (e.g., caterpillars, jellyfish), medications (e.g., cinnamic aldehyde, compound 48/80, dimethyl sulfoxide)
Immunologic or Uncertain Mechanism Contact Urticaria
Ammonium persulfate used in hair bleaches, chemicals, foods, textiles, wood, saliva, cosmetics, perfumes, bacitracin
Skin Diseases
Urticaria pigmentosa (mastocytosis), dermatitis herpetiformis, pemphigoid, amyloidosis
Hormones
Pregnancy, premenstrual flare-ups (progesterone)
Genetic, Autosomal Dominant (All Rare)
Hereditary angioedema, cholinergic urticaria with progressive nerve deafness, amyloidosis of the kidney, familial cold urticaria, vibratory urticaria
Acute Urticaria
If the urticaria has been present for less than 6 weeks, it is considered acute ( Fig. 6.11 ). The evaluation and management of acute urticaria are outlined in Box 6.4 . A history and physical examination should be performed, and laboratory studies are selected to investigate abnormalities. Histamine release that is induced by allergens (e.g., drugs, foods, or pollens) and mediated by IgE is a common cause of acute urticaria, and particular attention should be paid to these factors during the initial evaluation. There are no routine laboratory studies for the evaluation of acute urticaria. Once all possible causes are eliminated, the patient is treated with antihistamines to suppress the hives and stop the itching. Because urticaria clears spontaneously in most patients, an extensive workup is not advised during the early weeks of an urticarial eruption.


History and Physical Examination
- 1.
Ask the patient if he or she knows what causes the hives. In many instances, the patient will have determined the cause.
- 2.
Take a history. See Box 6.3 for specific etiologies. Drugs are common causes in adults. Viral respiratory tract infections and streptococcal infections are common causes in children.
- 3.
Perform a physical examination.
- 4.
Stroke the arm to test for dermographism.
If the etiology is not determined by history, physical examination, and stroking the arm, order laboratory tests.
Laboratory Tests
- 1.
Order complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), liver function tests (LFTs), and urinalysis.
- 2.
The history and physical examination may provide evidence that warrants additional tests. Consider testing for hepatitis A, B, or C; infectious mononucleosis; thyroid function; thyroid antibodies; and antinuclear antibodies (ANAs).
Consider Allergen Testing
- 1.
Skin tests: foods, drugs, aeroallergens, insect venom, natural rubber. Except for penicillin, antibiotics have a high false-positive rate with skin-prick testing.
- 2.
Radioallergosorbent tests (RASTs) for penicillin, succinylcholine, natural rubber latex.
- 3.
Food testing: food diaries and elimination diets.
- 4.
Oral challenge testing for food and food additives.
Management
- 1.
Avoid specific allergens.
- 2.
Treat with oral H 1 antagonists.
- 3.
Add H 2 antagonists for resistant cases.
- 4.
Anaphylaxis – subcutaneous epinephrine with or without parenteral H 1 and H 2 antihistamines (e.g., 50 mg of diphenhydramine and 50 mg of ranitidine). Systemic corticosteroids are sometimes useful.
- 5.
Intravenous contrast media reactions – pretreat with H 1 antagonists and corticosteroids.
- 6.
Latex allergic patients – prophylactic administration of corticosteroids before surgery.
- 7.
Insect venom reaction – desensitization, preloaded syringes of epinephrine.
Children With Hives.
Food origin is important in the etiology of infantile urticaria. In one series it accounted for 62% of patients, more than drug etiology (22%), physical urticaria (8%), and contact urticaria (8%).
Etiology of Acute Urticaria
Acute urticaria is IgE-mediated, complement-mediated, or nonimmune-mediated. The cause of acute urticaria is unknown in 30% to 50% of cases. The most common causes are infections, drugs, and foods (see Box 6.3 ).
IgE-Mediated Reactions.
Type I hypersensitivity reactions are probably responsible for most cases of acute urticaria. Circulating antigens such as foods, drugs, or inhalants interact with cell membrane–bound IgE to release histamine. Food allergies are present in 8% of children younger than 3 years of age and in 2% of adults. Food allergies are the most common cause of anaphylaxis. Yellow jackets are the most common cause of insect sting–induced urticaria/anaphylaxis in the United States. Latex-induced urticaria is an IgE-mediated reaction.
Complement-Mediated, or Immune Complex–Mediated, Acute Urticaria.
Complement-mediated acute urticaria can be precipitated by administration of whole blood, plasma, immunoglobulins, and drugs or by insect stings. Type III hypersensitivity reactions (Arthus reactions) occur with deposition of insoluble immune complexes in vessel walls. The complexes are composed of IgG or IgM with an antigen such as a drug. Urticaria occurs when the trapped complexes activate complement to cleave the anaphylatoxins C5a and C3a from C5 and C3. C5a and C3a are potent releasers of histamine from mast cells. Serum sickness (fevers, urticaria, lymphadenopathy, arthralgias, and myalgias), urticarial vasculitis, and systemic lupus erythematosus are diseases in which hives may occur as a result of immune complex deposition.
Nonimmunologic Release of Histamine.
Pharmacologic mediators, such as acetylcholine, opiates, polymyxin B, and strawberries, react directly with cell membrane–bound mediators to release histamine. Aspirin/nonsteroidal antiinflammatory drugs (NSAIDs) cause a nonimmunologic release of histamine. Patients with aspirin/NSAID sensitivity may have a history of allergic rhinitis or asthma. Urticaria may be caused by histamine-containing foods. Fish of the Scombridae family accumulate histamine during spoilage. The mechanism of radiocontrast-related urticaria/anaphylaxis is unknown. Incidence varies from 3.1% with newer, lower osmolar agents to 12.7% with previously established, higher osmolar agents. Atopy is a risk factor for urticaria developing after radiocontrast exposure. The physical urticarias may be induced both by direct stimulation of cell membrane receptors and by immunologic mechanisms.
Chronic Urticaria
Patients who have a history of hives lasting for 6 or more weeks are classified as having CU. The etiology is often unclear. The morphology is similar to that of acute urticaria ( Fig. 6.12 ). CU is more common in middle-aged women and is infrequent in children. Individual lesions remain for less than 24 hours, and any skin surface can be affected. Itching is worse at night. Respiratory and GI complaints are rare. Angioedema occurs in 50% of cases. Angioedema with CU differs from hereditary angioedema (HAE) in that it rarely affects the larynx and HAE patients do not have urticaria. CU patients may experience physical urticaria. Symptoms continue for weeks, months, or years. Pressure urticaria, CU, and angioedema frequently occur in the same patient. In one study, delayed pressure urticaria was present in 37% of patients with CU. Aspirin/NSAIDs, penicillin, angiotensin-converting enzyme inhibitors (ACEIs), opiates, alcohol, febrile illnesses, and stress exacerbate urticaria.

Pathogenesis
Chronic urticaria results from the cutaneous mast cell release of histamine. In contrast to acute urticaria, exogenous triggers are not found in most cases. Chronic urticaria in many cases may be an immune-mediated inflammatory disease. Release can be induced by specific immunoglobulin E (IgE), components of complement activation and endogenous peptides, endorphins, and enkephalins. Greater than 30% of CU patients have autoimmune phenomena characterized by positive ASSTs, antibodies to the alpha subunit of the basophil IgE receptor and to IgE, and thyroid autoimmunity. The evaluation and management of CU is outlined in Box 6.5 .
- 1.
CU is a diagnosis of exclusion
Determine that lesions are hives and not insect bites (see Table 6.2 for differential diagnosis). Individual bite lesion lasts longer than 24 hours. Hives last less than 24 hours. Most urticarial plaques are larger than 2 cm. Stroke the patient’s arm to rule out dermographism.
- 2.
Take a history
Exact time of onset
Medication
Food and drink
Duration
Acute – days to a few weeks
Chronic – more than 6 weeks
Time of appearance
Time of day
Time of year
Constant – food, internal disease
Seasonal – inhalant allergy
Environment
Exposure to pollens, chemicals
Home – clear while at work or on vacation
Work – contact or inhalation of chemicals
Appearance after physical stimuli (physical urticaria)
Scratching, pressure, exercise, sun exposure, cold
Associated with arthralgia and fever
Juvenile rheumatoid arthritis, rheumatic fever, serum sickness, systemic lupus erythematosus, urticarial vasculitis, viral hepatitis
Duration of individual lesion
Less than 1 hour – physical urticarias, typical hives
Less than 24 hours – typical hives
More than 25 hours – urticarial vasculitis; scaling and purpura as lesions resolve
- 3.
Physical examination
Stroke the arm to test for dermographism, and rule out other types of physical urticaria
Size
Papular – cholinergic urticaria, bites
Plaque – most cases
Thickness
Superficial – most cases
Deep – angioedema
Distribution
Generalized – ingestants, inhalants, internal disease
Localized – physical urticarias, contact urticaria
Sources of infection
Sinus and gum infections
Cystitis, vaginitis, prostatitis
Dental examination by dentist
Fix carious teeth
Treat periodontal disease
Internal disease, thyroid examination, gallbladder symptoms
If the etiology is not determined by history, physical examination, and stroking the arm, then consider ordering laboratory tests.
Laboratory Tests
- 1.
Initial screening tests are complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), liver function tests (LFTs), urinalysis, and studies to confirm findings of history and physical examination.
- 2.
Order screening thyroid function tests and tests for thyroid autoimmunity (thyroid microsomal and thyroglobulin antibodies), especially in women or in those patients with a family history of thyroid disease or other autoimmune diseases.
- 3.
Eosinophilia suggests drug, food, or parasitic causes.
- 4.
Leukocytosis suggests chronic infection.
- 5.
Order ANA and ESR for patients with connective tissue disease symptoms.
- 6.
Sinus radiographs have been advocated.
- 7.
Order oral challenge testing for food additives.
- 8.
Food testing: use food diaries and elimination diets.
- 9.
Perform lesion biopsy for hives lasting longer than 36 hours (rule out urticarial vasculitis), fever, arthralgias, elevated ESR, petechiae.
- 10.
Order C4 only for patients with angioedema (not for patients with hives).
Management (See Also Table 6.3 )
- 1.
Second-generation H 1 antihistamines: cetirizine (Zyrtec), loratadine (Claritin), fexofenadine (Allegra). Higher doses than suggested by the manufacturers may be required (e.g., 20 to 40 mg of cetirizine each day instead of 10 mg). Sedative side effects increase with higher dosages.
- 2.
Add H 2 antagonists if H 1 agents do not provide effective control.
- 3.
Hydroxyzine or doxepin is more sedating and can be added at nighttime. Doxepin can interact with other drugs that are metabolized by the cytochrome P-450 system (e.g., ketoconazole, itraconazole, erythromycin, clarithromycin).
- 4.
Systemic steroids (short courses) may be used to provide temporary relief.
- 5.
Stop vitamins, laxatives, antacids, toothpaste, cigarettes, cosmetics and all toiletries, chewing gum, household cleaning solutions, aerosols.
- 6.
Stop fruits, tomatoes, nuts, eggs, shellfish, chocolate, alcohol, milk, cheese, bread, diet drinks, junk food.
- 7.
Consider a highly restricted diet such as lamb, rice, and salt (rarely effective).
- 8.
Consider empiric treatment with antibiotics. Consider eradication of H. pylori in patients with infection.
- 9.
Leukotriene receptor antagonists – zafirlukast (Accolate 10 mg, 20 mg) and montelukast (Singulair 10 mg/day) – may be effective, especially in combination with antihistamines. Leukotriene receptor antagonists may prevent the severe urticaria/angioedema exacerbations that follow the use of nonsteroidal antiinflammatory drugs (NSAIDs) in some patients with chronic urticaria.
- 10.
Cyclosporine – patients with severe, unremitting chronic urticaria that responded poorly to antihistamines responded to cyclosporine 4 mg/kg daily in combination with cetirizine 20 mg daily.
- 11.
Omalizumab – patients 12 years and older with chronic idiopathic urticaria who fail H 1 antihistamines. Omalizumab is dosed subcutaneously 150 or 300 mg every 4 weeks.
The patient must understand that the course of this disease is unpredictable; it may last for months or years. During the evaluation, the patient should be assured that antihistamines will decrease discomfort. The patient should also be told that although the evaluation may be lengthy and is often unrewarding, in most cases the disease ends spontaneously. Patients who understand the nature of this disease do not become discouraged so easily, nor are they as apt to go from physician to physician seeking a cure.
There are many studies in the literature on CU. Most demonstrate that if the cause is not found after investigation of abnormalities elicited during the history and physical examination, there is little chance that it will be determined. It is tempting to order laboratory tests such as antinuclear antibody (ANA) levels and stool examinations for ova and parasites in an effort to be thorough, but results of studies do not support this approach. There are certain tests and procedures that might be considered when the initial evaluation has proved unrewarding.
Rule Out Physical Urticarias.
Unrecognized physical urticarias (see p. 189 ) may account for approximately 10% of all cases of CU. In one large study physical urticarias were present in 71% of patients with CU: 22% had immediate dermographism, 37% had delayed pressure urticaria, 11% had cholinergic urticaria, and 2% had cold urticaria.
The presence of physical urticaria should be ruled out by history and appropriate tests before a lengthy evaluation and treatment program is undertaken. Dermographism is the most common type of physical urticaria; it begins suddenly following drug therapy or a viral illness, persists for months or years, and clears spontaneously. Wheals that appear after the patient’s arm is stroked prove the diagnosis.
Thyroid Autoimmune Disease.
There is a significant association between CU and autoimmune thyroid disease (Hashimoto thyroiditis, Graves disease, toxic multinodular goiter). Thyroid autoimmunity was found in 12% of 140 consecutively seen patients with CU in one series; 88% were women. Most patients with thyroid autoimmunity are asymptomatic and have thyroid function that is normal or only slightly abnormal. Guidelines for evaluation and treatment of thyroid-related urticaria are presented in Box 6.6 .
- 1.
Screen for thyroid autoimmunity by testing for thyroid microsomal and thyroglobulin antibodies, especially in women (female:male ratio was 7 : 1), or in those patients with a family history of thyroid disease or other autoimmune disorders.
- 2.
The administration of thyroid hormone may alleviate chronic urticaria and/or angioedema in selected patients.
If patients with documented thyroid autoimmunity have been unresponsive to standard therapy for chronic urticaria and/or angioedema, consider the use of levothyroxine if the patients are hypothyroid or euthyroid. An appropriate initial dose is 1.7 mcg/kg/day.
- 3.
The level of thyroid-stimulating hormone should be monitored by weeks 4 to 6 after the initiation of therapy, being kept in the low–normal range, to ensure that the patient is not becoming hyperthyroid.
- 4.
If there has been no response of the chronic urticaria and/or angioedema by week 8 of administration, levothyroxine should be discontinued.
- 5.
After being in remission for at least 1 to 2 months, levothyroxine should be discontinued. Should the chronic urticaria and/or angioedema recur, the hormone may be readministered, with an expectation that most patients will again be responsive to treatment.
Differential Diagnosis
The differential diagnosis of CU includes diseases that have lesions that mimic urticaria ( Table 6.2 ). These often have fixed urticarial lesions that have some atypical features, such as duration greater than 24 hours, relative lack of itch, or presence of epithelial changes (e.g., hyperpigmentation or hypopigmentation, vesicles or blisters, or scaling).
| Cutaneous lupus erythematosus | Subacute cutaneous lupus erythematosus can present with urticarial-like lesions that burn rather than itch. |
| Urticarial vasculitis | A small- to medium-vessel leukocytoclastic vasculitis, urticarial wheals; up to 40% have angioedema. Lesions are painful or burn, last several days, heal with dyspigmentation or purpura. Urticarial vasculitis is a harbinger of more active disease. |
| Urticaria pigmentosa | Orange to deep brown pigmentation overlying the wheal. Urtication produced by stroking the skin; spares face, scalp, palms, and soles. |
| Sweet syndrome | Women 30 to 50 years of age, acute fever, leukocytosis, urticarial-like plaques that may resemble urticaria, but are more persistent. Some lesions are studded with papules. |
| Fixed drug eruption | Lesions occur in the same spot (or spots) with each exposure to offending agent. Red macule becomes edematous and develops hyperpigmentation. |
| Bullous pemphigoid | In this autoimmune, subepidermal blistering disease, blisters appear on urticarial plaques. |
| Muckle–Wells syndrome (urticaria–deafness– amyloidosis syndrome) | Symptoms include recurrent urticarial lesions, fever, arthralgia, arthritis, malaise, conjunctivitis, sensorineural hearing loss, secondary amyloidosis. |
| Chronic infantile neurologic cutaneous articular syndrome (neonatal-onset multisystemic inflammatory disease) | Characteristics include (1) neonatal onset of cutaneous symptoms, (2) chronic meningitis, and (3) joint manifestations with recurrent fever and inflammation. |
| Schnitzler syndrome | Symptoms include chronic, nonpruritic urticaria, fever, arthralgias or arthritis, bone pain, lymphadenopathy, immunoglobulin G (IgG) gammopathy. |
Change of Environment.
Because the environment consists of numerous antigens, patients should consider a trial period of 1 or 2 weeks of separation from home and work, preferably with a geographic change.
Highly Restricted Diet.
A highly restricted diet may be attempted. Patients are fed lamb, rice, sugar, salt, and water for 5 days. The occurrence of new hives after 3 days suggests that foods have no role. If hives disappear, a new food is reintroduced every other day until hives appear.
Treatment of Occult Infections.
Patients occasionally respond to antibiotics even in the absence of clinical infection. Consider eradication of Helicobacter pylori in patients with infection.
Skin Biopsy.
Urticarial reactions display a wide spectrum of changes, ranging from a mild, mixed dermal inflammatory response to true vasculitis. Patients with hives that are characteristic of urticarial vasculitis should have a biopsy taken of the urticarial plaque. These hives burn rather than itch and last longer than 24 hours.
Dermal edema and dilated lymphatic and vascular capillaries occur. Increased numbers of neutrophils and eosinophils occur in patients with acute urticaria and in those with delayed pressure urticaria. Mast cell numbers are higher in the dermis of lesional and uninvolved skin of all patients with urticaria. Mononuclear infiltrates are more pronounced in cold urticaria and CU, when compared with other forms of CU.
Treatment of Urticaria
Table 6.3 lists the medications used to treat urticaria.
Approach to Treatment
First-Line Therapy
Nonsedating H 1 antihistamines (e.g., fexofenadine 180 mg daily) are the first choice for treatment. Previously established sedating H 1 antihistamines are more effective and so should be used to treat severe urticaria (e.g., 100 to 200 mg of hydroxyzine or diphenhydramine per day). For patients with severe angioedema (involving swelling of the face, tongue, and pharynx), diphenhydramine is particularly effective.
Patients become accustomed to the sedating effects after about a week, but their performance on driving tests remains impaired. H 2 -receptor antagonists have very few side effects and may be useful as adjunctive therapy. Leukotriene antagonists (montelukast 10 mg per day) are considered safe and are worth trying, but severe disease may require prednisone; many regimens have been suggested.
One approach is to start prednisone at 15 to 20 mg as a single morning dose every other day, gradually tapering to 2.5 to 5 mg every 3 weeks, depending on the patient’s response, and discontinue after 4 to 5 months. Side effects are minimized with the use of dietary discretion and exercise. Some patients require a combination of all of these medications.
Patients who have no response to any of these approaches may respond to cyclosporine (200 to 300 mg of cyclosporine per day) or methotrexate (15 mg/week).
Antihistamines.
For the majority of patients, acute and chronic urticaria may be controlled with antihistamines.
Mechanism of Action.
Antihistamines control urticaria by inhibiting vasodilation and vessel fluid loss. Antihistamines do not block the release of histamine. If histamine has been released before an antihistamine is taken, the receptor sites will be occupied and the antihistamine will have no effect.
Initiation of Treatment.
Antihistamines are the preferred initial treatment for urticaria and angioedema. Cetirizine, loratadine, or fexofenadine are first-line agents and are given once daily. Higher doses than suggested by the manufacturers may be required; see Table 6.3 for medications to treat urticaria. Patients with daytime and nighttime symptoms can be treated with combination therapy. These patients can be treated with a low-sedating antihistamine in the morning (e.g., loratadine 10 mg, or fexofenadine 180 mg, or cetirizine 10 to 20 mg) and a sedating antihistamine (e.g., hydroxyzine 25 mg) in the evening. Cetirizine can be mildly sedating. Doxepin is an alternative bedtime medication especially effective for anxious or depressed patients. The initial dose is 10 to 25 mg. Gradually increase the dose up to 75 mg for optimal control. Some patients with CU respond when an H 2 -receptor antagonist such as cimetidine is added to conventional antihistamines. This may be worth trying in refractory cases.
Side Effects.
Antihistamines are structurally similar to atropine; therefore they produce atropine-like peripheral and central anticholinergic effects such as dry mouth, blurred vision, constipation, and dizziness. First-generation antihistamines (H 1 -receptor antagonists) such as chlorpheniramine, hydroxyzine, and diphenhydramine cross the blood–brain barrier and produce sedation. There is marked individual variation in response and side effects. Antihistamines may produce paradoxical psychomotor stimulation in children, especially in those ages 6 through 12.
Long-Term Administration.
Prolonged use of H 1 antagonists does not lead to autoinduction of hepatic metabolism. The efficacy of H 1 -receptor blockade does not decrease with prolonged use. Tolerance of adverse central nervous system effects may or may not develop.
H 1 and H 2 Antihistamines.
The majority of available antihistamines are H 1 antagonists (i.e., they compete for the H 1 -receptor sites). Cimetidine, ranitidine, and famotidine are H 2 antagonists that are used primarily for the treatment of gastric hyperacidity. Approximately 85% of histamine receptors in the skin are the H 1 subtype, and 15% are H 2 receptors. The addition of an H 2 -receptor antagonist to an H 1 -receptor antagonist augments the inhibition of a histamine-induced wheal-and-flare reaction once H 1 -receptor blockade has been maximized. It would seem that the combination of H 1 and H 2 antihistamines would provide optimal effects. The results of studies are conflicting but generally show that the combination is only slightly more effective than an H 1 -blocking agent used alone.
First-Generation (Sedating) H 1 Antihistamines.
The first-generation H 1 antihistamines are divided into five classes (see Table 6.3 ). They are lipophilic, cross the blood–brain barrier, cause sedation, weight gain, and atropine-like complications including dry mouth, blurred vision, constipation, and dysuria. Metabolism occurs via the hepatic cytochrome P-450 (CYP) system. In patients with liver disease, or in patients who are taking CYP 3A4 inhibitors such as erythromycin or ketoconazole, the plasma half-life may be prolonged. The H 1 antagonists suppress the wheal caused by histamine. Antihistamines given during or after the onset of a hive are less effective. They prevent wheals rather than treat them.
Second-Generation (Low-Sedating) H 1 Antihistamines.
The second-generation antihistamines are not lipophilic and do not readily cross the blood–brain barrier. They cause little sedation and little or no atropine-like activity.
Fexofenadine (Allegra).
Fexofenadine in a single dose of 180 mg daily or 60 mg twice daily is the recommended dosage for treating urticaria. Dosage adjustment is not necessary in the elderly or in patients with mild renal or hepatic impairment. Fexofenadine may offer the best combination of effectiveness and safety of all of the low-sedating antihistamines. A dose that is higher than recommended may be required.
Cetirizine (Zyrtec).
Cetirizine is a metabolite of the first-generation H 1 -antihistamine hydroxyzine. Some patients notice drowsiness after a 10-mg dose. The adult dose is 10 mg daily. A reduced dosage (5 mg daily) is recommended in patients with chronic renal impairment. No drug interactions are reported, and there is no cardiotoxicity. A dose higher than recommended may be required. Adverse effects on behavior and learning do not occur with long-term use of cetirizine in young children.
Levocetirizine (Xyzal).
Levocetirizine (5-mg tablets and oral solution [0.5 mg/mL]) is the R enantiomer of cetirizine. This drug has similar H 1 -antihistamine activity to cetirizine and yet is less sedating. Patients 12 years of age and older take 5 mg daily, 6 to 11 years take 2.5 mg daily. Dosage adjustments must be made in patients with renal impairment.
Loratadine (Claritin).
Loratadine is a long-acting second-generation H 1 -histamine antagonist. A 10-mg dose suppresses whealing for up to 12 hours; suppression lasts longer after a larger dosage. A reduced dosage may be required in patients with chronic liver or renal disease. There are no significant adverse drug interactions. A special form of the medication, RediTabs (10 mg), rapidly disintegrates in the mouth. A dose higher than recommended may be required.
Desloratadine (Clarinex).
Desloratadine is an active metabolite of loratadine. A 5-mg dose each day is effective. There is no evidence that it offers any advantage over loratadine.
Tricyclic Antihistamines (Doxepin).
Tricyclic antidepressants are potent blockers of histamine H 1 and H 2 receptors. The most potent is doxepin. When taken in dosages between 10 and 25 mg three times a day, doxepin is effective for the treatment of chronic idiopathic urticaria. Few side effects occur at this low dosage. Higher dosages may be tolerated if taken in the evening. Doxepin is a good alternative for patients with CU not controlled with conventional antihistamines and for patients who suffer anxiety and depression associated with CU. Lethargy is commonly observed but diminishes with continued use. Dry mouth and constipation are also commonly observed. Doxepin can interact with other drugs that are metabolized by the cytochrome P-450 system (e.g., ketoconazole, itraconazole, erythromycin, clarithromycin).
Epinephrine.
Severe urticaria or angioedema requires epinephrine. Epinephrine solutions have a rapid onset of effect but a short duration of action. The dosage for adults is a 1 : 1000 solution (0.2 to 1.0 mL) given either subcutaneously or intramuscularly; the initial dose is usually 0.3 mL. The epinephrine suspensions provide both a prompt and a prolonged effect (up to 8 hours). For adults, 0.1 to 0.3 mL of the 1 : 200 suspension is given subcutaneously.
Second-Line Agents
Oral Corticosteroids.
Many patients with CU and angioedema will have little response to even a combination of H 1 – and H 2 -receptor blockers. Oral corticosteroids should be considered for these refractory cases. Because of toxicity, corticosteroids are reserved for antihistamine failures or the most severe cases. They are reliable and effective. They do not have the potential for drug-free remission. Prednisone 40 mg/day given in a single morning dose or 20 mg twice a day is effective in most cases. Another approach is to prescribe thirty 20-mg tablets. The patient receives 5 days each of 60 mg, 40 mg, and 20 mg, and the medication is taken once each morning. Others will respond to prednisone 20 mg every other day with a gradual taper.
Leukotriene Modifiers.
Leukotriene modifiers may provide improvement in some cases of antihistamine-resistant CU. Excellent safety, absence of required monitoring in the cases of montelukast and zafirlukast, and wide availability make leukotriene modifiers the preferred alternative agent. Montelukast, zafirlukast, and zileuton have been studied. Response may take days to weeks. Randomized controlled trials show zafirlukast and montelukast either singly or in combination with antihistamines are effective but several negative studies have also appeared. Montelukast was demonstrated to be effective for patients with NSAID-exacerbated CU. Patients with positive autologous serum skin test (ASST) results may predict better response to leukotriene modifiers. Experience in physical urticarias has also been promising.
Dapsone.
Small studies demonstrate excellent clinical response with dosages that vary from 25 mg/day to 100 mg/day. Response may be fairly rapid, but some patients require several weeks to notice improvement. Monitor for the predictable small decline in hemoglobin level. The drug is generally well tolerated. There is a possibility of sustained remission after stopping the drug. Obtain a glucose-6-phosphate dehydrogenase (G6PD) level to avoid more severe hemolytic anemia in G6PD-deficient patients.
Cyclosporine.
Cyclosporine might be an effective alternative in some CU patients unresponsive to conventional treatments and may be considered if leukotriene modifiers and dapsone fail. Patients with severe unremitting disease who respond poorly to antihistamines may respond to cyclosporine 4 mg/kg daily for 4 weeks. Patients requiring initially high doses of glucocorticosteroids and with a long clinical history are less amenable to cyclosporine treatment.
Mycophenolate Mofetil.
Mycophenolate mofetil (MMF) is a useful and well-tolerated second-line therapy for patients with autoimmune and chronic idiopathic urticaria in whom antihistamines and other therapeutic agents have failed. Combining MMF with oral prednisolone was helpful in gaining immediate control of the CU symptoms.
Third-Line Agents
Intravenous Immunoglobulin.
Responses ranging from complete and lasting remission to modest transient benefit are reported. Response seems to be rapid. The optimal dose and number of infusions to attempt are unclear. Only case reports and short series of patients are reported.
Methotrexate.
Methotrexate may be considered in resistant cases of urticaria. Case reports and a small series of patients document benefit within 1 to 2 weeks of starting methotrexate. Because adverse effects may be serious and frequent monitoring is necessary, methotrexate should be reserved for intractable cases in which other alternative agents have failed. Methotrexate 10 to 15 mg weekly has been successful.
Topical Measures.
Itching is controlled with tepid showering, tepid oatmeal baths (Aveeno), cooling lotions that contain menthol (Sarna lotion), and topical pramoxine lotions (Itch-X). Avoid factors that enhance pruritus (e.g., taking aspirin, drinking alcohol, or wearing tight elasticized apparel or coarse woolen fabrics).
Omalizumab (Xolair).
Omalizumab, a recombinant humanized monoclonal antibody (IgG1κ) that selectively binds to human IgE, reduces the levels of free IgE and the high-affinity receptor for the Fc region of IgE (FcεRI), both of which are essential in mast cell and basophil activation. Omalizumab is indicated for chronic idiopathic urticaria in adults and children older than 12 years of age. It is administered 150 mg or 300 mg by monthly subcutaneous injections. The dosing for chronic idiopathic urticaria is not dependent on serum IgE or body weight.
Physical Urticarias
Physical urticarias are induced by physical and external stimuli, and they typically affect young adults. More than one type of physical urticaria can occur in an individual. Provocative testing confirms the diagnosis. During the initial examination, the physician should determine whether the hives are elicited by physical stimuli ( Table 6.4 ). Patients with these distinctive hives may be spared a detailed laboratory evaluation; they simply require an explanation of their condition and its treatment. Unrecognized physical urticarias may account for approximately 20% of all cases of CU. A major distinguishing feature of the physical urticarias is that attacks are brief, lasting only 30 to 120 minutes. In typical urticaria, individual lesions last from hours to a few days. The one exception among physical urticarias is pressure urticaria, in which swelling may last several hours. Most physical urticaria forms persist for about 3 to 5 years or longer.
| Clinical Features | |
|---|---|
| PU SUBTYPE | CLINICAL PICTURE |
| Dermographism | Linear wheals from shear force, often localized to sites of pressure by clothing, shoes, underwear, belts. Also sites of trauma, friction, or scratching. |
| Delayed pressure urticaria | Pruritus, swelling, and pain 4–12 h after exposure to pressure. |
| Cold contact urticaria | Wheals, erythema, and itch after exposure/contact with cold air, liquids or objects. |
| Heat contact urticaria | Reaction limited to area of exposure to heat. |
| Solar urticaria | Immediate reaction consistent of wheals on areas of skin exposed to sunlight (UV and visible light). |
| Vibratory urticaria | Erythema and swelling at the site of vibratory stimulus. |
| Diagnostic Methods Useful to Investigate Patients With Physical Urticarias | |
| PU SUBTYPE | DIAGNOSTIC METHODS |
| Dermographism | Stroking the skin with a wooden spatula or ball-point pen Fric test Dermographometer |
| Delayed pressure urticaria | 7 kg weight bearing on shoulder or lower leg for 15–20 mins Dermographometer |
| Cold contact urticaria | Wheal and flare with pruritus from contact with cold object (“ice-cube test”) TempTest Hand immersion in 10° C water bath for 5 mins |
| Heat contact urticaria | Hot water (45–50° C) in glass beaker for 1–10 mins |
| Solar urticaria | Phototesting |
| Vibratory urticaria | Vibratory stimulation for 1–5 mins with vortex |
Dermographism
Also known as “skin writing,” dermographism is the most common physical urticaria, occurring to some degree in approximately 5% of the population. Scratching, toweling, or performing other activities that produce minor skin trauma induce itching and wheals. The onset is usually sudden; young patients are affected most commonly. The tendency to be dermographic lasts for weeks to months or years. The condition has an average course of 2 to 3 years before resolving spontaneously. It may be preceded by a viral infection, antibiotic therapy (especially penicillin), or emotional upset, but in most cases the cause is unknown. Mucosal involvement and angioedema do not occur. There are no recognized systemic associations (such as atopy or autoimmunity).
The degree of urticarial response varies. A patient will be highly reactive for months and then appear to be in remission, only to have symptoms recur ( Fig. 6.13 ). Patients complain of linear, itchy wheals from scratching or wheals at the site of friction from clothing. Delayed dermographism, in which the immediate urticarial response is followed in 1 to 6 hours by a wheal that persists for 24 to 48 hours, is rare.

Diagnosis.
A tongue blade drawn firmly across the patient’s arm or back produces whealing 2 mm or more in width in approximately 1 to 3 minutes (Darier’s sign), an exaggerated triple response ( Fig. 6.14 ).
- 1.
A red line occurs in 3 to 15 seconds (capillary dilation).
- 2.
Broadening erythema appears (axon reflex flare from arteriolar dilation).
- 3.
A wheal with surrounding erythema replaces the red line (transudation of fluid through dilated capillaries).

Unlike urticaria pigmentosa caused by cutaneous mastocytosis (CM; which also manifests dermographism – Darier’s sign), there is no increase in skin mast cell numbers.
Treatment.
Treatment is not necessary unless the patient is highly sensitive and reacts continually to the slightest trauma. Antihistamines are very effective. Nonsedating H 1 antihistamines or hydroxyzine in relatively low dosages (10 to 25 mg daily one to four times a day) provides adequate relief. Some patients are severely affected and require continuous suppression. Use the lowest dose possible to stop itching. Many patients adapt to a low dose of hydroxyzine and do not feel sedated.
Pressure Urticaria
A deep, itchy, burning, or painful swelling occurring 2 to 6 hours after a pressure stimulus and lasting 8 to 72 hours is characteristic of this common form of physical urticaria. The mean age of onset is the early thirties. The disease is chronic, and the mean duration is 9 years (range: 1 to 40 years). Malaise, fatigue, fever, chills, headache, or generalized arthralgia may occur. Many of those affected have moderate to severe disease that is disabling, especially for those who perform manual labor. Pressure urticaria, CU, and angioedema frequently occur in the same patient. In one study delayed pressure urticaria was present in 37% of patients with CU. This explains the frequency of wheals at local pressure sites in patients with CU. It also explains the poor response to H 1 antihistamines in some patients because delayed pressure urticaria is generally poorly responsive to this treatment.
The hands, feet, trunk, buttocks, lips, and face are commonly affected. Lesions are induced by standing, walking, wearing tight garments, or prolonged sitting on a hard surface ( Figs. 6.15 and 6.16 ).










