Key Words
atopic dermatitis, xerosis, pityriasis, food allergy, topical steroids, antihistamines, diffuse inflammation, keratosis pilaris, ichthyosis vulgaris, contact allergy
The term atopy was introduced years ago to designate a group of patients who had a personal or family history of one or more of the following diseases: hay fever, asthma, very dry skin, and eczema.
Atopic dermatitis (AD) is a chronic, pruritic inflammatory skin disease that occurs most frequently in children, but also affects many adults. It follows a relapsing course. AD is often associated with elevated serum immunoglobulin E (IgE) levels and a personal or family history of type I allergies, allergic rhinitis, and asthma. Atopic eczema is synonymous with AD.
The disease characteristics vary with age. Infants have facial and patchy or generalized body eczema. Adolescents and adults have eczema in flexural areas and on the hands. The pattern of inheritance is unknown, but available data suggest that it is polygenic.
Diagnostic Criteria.
There are no specific cutaneous signs, no known distinctive histologic features, and no characteristic laboratory findings for AD. There are a variety of characteristics that indicate that the patient has AD ( Box 5.1 ).
Essential Features
Must be present:
- •
Pruritus
- •
Eczema (acute, subacute, chronic)
Typical morphology and age-specific patterns*
Chronic or relapsing history
*Patterns include:
- 1.
Facial, neck, and extensor involvement in infants and children
- 2.
Current or previous flexural lesions in any age group
- 3.
Sparing of the groin and axillary regions
Important Features
Seen in most cases, adding support to the diagnosis:
- •
Early age of onset
- •
Atopy
Personal and/or family history
Immunoglobulin E reactivity
- •
Xerosis
Associated Features
These clinical associations help to suggest the diagnosis of atopic dermatitis but are too nonspecific to be used for defining or detecting atopic dermatitis for research and epidemiologic studies:
- •
Atypical vascular responses (e.g., facial pallor, white dermographism, delayed blanch response)
- •
Keratosis pilaris/pityriasis alba/hyperlinear palms/ichthyosis
- •
Ocular/periorbital changes
- •
Other regional findings (e.g., perioral changes/periauricular lesions)
- •
Perifollicular accentuation/lichenification/prurigo lesions
Exclusionary Conditions
It should be noted that a diagnosis of atopic dermatitis depends on excluding conditions, such as:
- •
Scabies
- •
Seborrheic dermatitis
- •
Contact dermatitis (irritant or allergic)
- •
Ichthyoses
- •
Cutaneous T-cell lymphoma
- •
Psoriasis
- •
Photosensitivity dermatoses
- •
Immune deficiency diseases
- •
Erythroderma of other causes
Prevalence.
The prevalence of AD is increasing. Fifteen to 25% of children and 7.2% of adults are affected in the United States. The increase in prevalence is thought to be due to microbe exposure during infancy and childhood. Some studies show that AD is less prevalent in rural areas. About 45% of cases of AD begin within the first 6 months of life, 60% begin during the first year, and 85% begin before 5 years of age. Genetic factors cannot explain the rapid change in prevalence. Changes in environmental factors and lifestyle, as well as increased recognition of the disease by physicians and families, are contributory factors. Some events in childhood may be of importance (e.g., early infections, early allergen exposure, and early diet).
Genetics.
The concordance rate for AD is higher among monozygotic twins (77%) than among dizygotic twins (15%). Allergic asthma or allergic rhinitis in a parent is a minor factor in the development of AD in the offspring. Studies show that asthma, hay fever, and AD coexist because they share a common genetic origin. Multiple genes are involved in the pathogenesis of AD. The interaction of these genes with the environment determines the incidence and course of AD.
Course and Prognosis
Factors associated with a low frequency of healing and increased severity of persistent or recurring dermatitis are listed in order of relative importance in Box 5.2 . More than 50% of young children with generalized AD develop asthma and allergic rhinitis by the age of 13. Infants who develop AD before the age of 2 tend to have a shorter disease course. Up to 80% of children show improvement before 8 years of age, but many continue to have difficulties with their skin into adulthood . The notion that children outgrow AD should be abandoned, since this statement does not account for the complex mechanisms of disease and the many behavioral and environmental factors that determine disease course. Older age of onset and more severe disease are positive predictors of a prolonged AD course. Atopic dermatitis starting in adulthood may be very difficult to control.
Persistent dry or itchy skin in adult life
Widespread dermatitis in childhood
Associated allergic rhinitis
Family history of atopic dermatitis
Associated bronchial asthma
Female gender
Seventy percent of atopic patients have a family history of one or more of the major atopic characteristics: asthma, hay fever, or eczematous dermatitis.
Misconceptions.
There are two common misconceptions about AD. The first is that it is an emotional disorder. It is true that patients with inflammation that lasts for months or years seem to be irritable, but this is a normal response to a frustrating disease. The second misconception is that atopic skin disease is precipitated by an allergic reaction. Atopic individuals frequently have respiratory allergies and, when skin tested, are informed that they are allergic to “everything.” Atopic patients may react with a wheal when challenged with a needle during skin testing, but this is a characteristic of atopic skin and is not necessarily a manifestation of allergy. All evidence to date shows that most cases of AD are precipitated by environmental stress on genetically compromised skin and not by interaction with allergens.
Pathogenesis and Immunology
Intrinsic versus Extrinsic AD.
Patients with intrinsic AD do not have elevated IgE levels and filaggrin (FLG) mutations. Intrinsic AD begins in adulthood and the immune system exhibits TH-17 and TH-22 activation. Patients with extrinsic AD have elevated levels of IgE, FLG mutations, early onset AD, and a TH-2 dominant immune response.
The Epidermal Permeability Barrier, Skin Microbiome, and Immunity.
Disruption of the epidermal permeability barrier and alteration in innate and adaptive immune responses are important in the pathophysiology of AD. Filaggrin (filament aggregating protein) is found in the upper layers of the skin and is altered in many patients with AD. Filaggrin levels may be decreased due to loss of function mutations in the FLA gene or due to inflammation reducing the expression of filaggrin. Decreased filaggrin function results in alterations in lipid lamellae formation, leading to increased skin permeability. Diminished skin barrier function directly leads to a decrease in bacterial (microbiome) strain diversity. Children with more severe AD have greater Staphylococcus aureus (especially clonal strains), while children with less severe disease have more Staphylococcus epidermidis . Lesional skin in patients with AD shows strong activation of TH-2 cytokines (overexpression of IL-4, IL-5, IL-13). Increased levels of TH-2 cytokines alter host innate immunity (reduced expression of Toll-like receptors and antimicrobial peptides) and down-regulate proteins important for barrier function (filaggrin, loricrin, and involucrin).
Pruritus.
The underlying mechanism of itch is multifactorial, involving hyperinnervation of the epidermis and lower activation thresholds of sensory nerves. Histamine (H1, H4 receptors), protease (tryptase, dust mites, and S. aureus ), substance P, TSLP (thymic stromal lymphopoietin), endothelin-1, IL-31 signaling, and alteration in the central nervous system (altered interpretation and perception of itch) are factors known to be important in AD pruritus. Future therapies will target these pathways.
Elevated IgE and the Inflammatory Response.
The role of IgE in AD is unknown. The IgE level is increased in the serum of many patients with AD, but 20% of AD patients have normal serum IgE levels and no allergen reactivity. The levels of IgE do not necessarily correlate with the activity of the disease; therefore elevated serum IgE levels can only be considered supporting evidence for the disease. Total IgE level is significantly higher in children with coexistent atopic respiratory disease in all age groups. Most people with AD have a personal or family history of allergic rhinitis or asthma and increased levels of serum IgE antibodies against airborne or ingested protein antigens. AD usually diminishes during the spring hay fever season, when aeroallergens are at maximum concentrations.
Blood Eosinophilia.
Eosinophils may be major effector cells in AD. Blood eosinophil counts roughly correlate with disease severity, although many patients with severe disease show normal peripheral blood eosinophil counts. Patients with normal eosinophil counts mainly are those with AD alone; patients with severe AD and concomitant respiratory allergies commonly have increased concentrations of peripheral blood eosinophils. There is no accumulation of tissue eosinophils; however, degranulation of eosinophils in the dermis releases major basic protein that may induce histamine release from basophils and mast cells and stimulate itching, irritation, and lichenification.
Reduced Cell-Mediated Immunity.
Several facts suggest that AD patients have disordered cell-mediated immunity. Patients may develop severe diffuse cutaneous infection with the herpes simplex virus (eczema herpeticum) whether or not their dermatitis is active. Mothers with active herpes labialis should avoid direct contact of their active lesion with their children’s skin, as in kissing, especially if the child has dermatitis. The incidence of contact allergy (e.g., reduced sensitivity to poison ivy) may be lower than normal in atopic patients; however, some studies show equal rates of sensitization. Humoral immunity seems to be normal.
Aeroallergens.
Aeroallergens may play an important role in causing eczematous lesions. Patch-testing rates of reactions are the following: house dust, 70%; mites, 70%; cockroaches, 63%; mold mix, 50%; and grass mix, 43%. Patients with AD frequently show positive scratch and intradermal reactions to a number of antigens; avoidance of these antigens rarely improves the dermatitis.
Clinical Aspects
Major and Minor Diagnostic Features.
Box 5.1 (the criteria for diagnosing AD) lists the major and minor diagnostic features for AD and atopy. Each patient has his or her own unique set of features, and there is no precise clinical or laboratory marker for this genetic disease.
Itching, the Primary Lesion.
“It is not the eruption that is itchy but the itchiness that is eruptive.” Atopic dermatitis starts with itching. Abnormally dry skin and a lowered threshold for itching are important features of AD. It is the scratching that creates most of the characteristic patterns of the disease. Most patients with AD make a determined effort to control their scratching, but during sleep, conscious control is lost; under warm covers the patient scratches and a rash appears. The itch–scratch cycle is established, and conscious effort is no longer sufficient to control scratching. The act of scratching becomes habitual, and the disease progresses. Atopic skin is associated with a lowered threshold of responsiveness to irritants.
Patterns of Inflammation.
Several patterns and types of lesions may be produced by exposure to external stimuli or may be precipitated by scratching. Acute inflammation begins with erythematous papules and erythema. These are associated with excoriations, erosions, and serous exudate. Subacute dermatitis is associated with erythematous, excoriated scaling papules. Chronic dermatitis is the result of scratching over an extended period, resulting in thickened skin, accentuated skin markings (lichenification), and fibrotic papules. Inflammation resolves slowly, leaving the skin in a dry, scaly compromised condition called xerosis. There is no single primary lesion in AD. All three types of reactions can coexist in the same individual. These types of lesions are eczematous dermatitis with redness and scaling ( Fig. 5.1 ), papules ( Fig. 5.2 ![]() ), and lichenification ( Fig. 5.3 ). Lichenification represents a thickening of the epidermis. It is a highly characteristic lesion, with the normal skin lines accentuated to resemble a washboard. These responses are altered by excoriation and infection.
), and lichenification ( Fig. 5.3 ). Lichenification represents a thickening of the epidermis. It is a highly characteristic lesion, with the normal skin lines accentuated to resemble a washboard. These responses are altered by excoriation and infection.



Although the cutaneous manifestations of the atopic diathesis are varied, they have characteristic age-determined patterns. Knowledge of these patterns is useful; many patients, however, have a nonclassic pattern. AD may terminate after an indefinite period or may progress from infancy to adulthood with little or no relief; 58% of infants with AD were found to have persistent inflammation 15 to 17 years later. AD is arbitrarily divided into three phases.
Infant Phase (Birth to 2 Years)
Infants are rarely born with atopic eczema, but they typically develop the first signs of inflammation during the third month of life. The most common occurrence is that of a baby who during the winter months develops dry, red scaling areas confined to the cheeks, but sparing the perioral and paranasal areas ( Figs. 5.4 to 5.9 ![]() ). This is the same area that becomes flushed with exposure to cold. The chin is often involved and initially may be more inflamed than the cheeks because of the irritation of drooling and subsequent repeated washing. Inflammation may spread to involve the paranasal and perioral area as the winter progresses. Habitual lip licking by an atopic child results in oozing, crusting, and scaling on the lips and perioral skin ( Figs. 5.10 and 5.11 ).
). This is the same area that becomes flushed with exposure to cold. The chin is often involved and initially may be more inflamed than the cheeks because of the irritation of drooling and subsequent repeated washing. Inflammation may spread to involve the paranasal and perioral area as the winter progresses. Habitual lip licking by an atopic child results in oozing, crusting, and scaling on the lips and perioral skin ( Figs. 5.10 and 5.11 ).

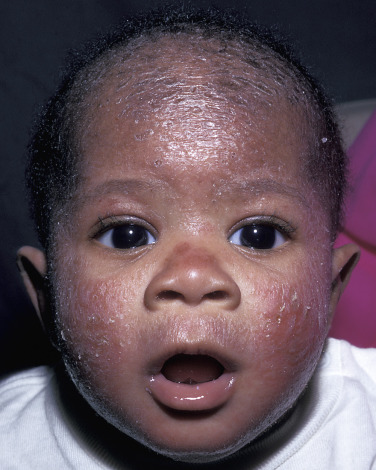







Many infants do not excoriate during these early stages, and the rash remains localized and chronic. Repeated scratching or washing creates red, scaling, oozing plaques on the cheeks, a classic presentation of infantile eczema. At this stage the infant is uncomfortable and becomes restless and agitated during sleep.
A small but significant number of infants have a generalized eruption consisting of papules, redness, scaling, and areas of lichenification. Lichenification may occur in the fossae and crease areas, or it may be confined to a favorite, easily reached spot, such as directly below the diaper, the back of the hand, or the extensor forearm ( Figs. 5.12 to 5.15 ![]() ). The scalp may be involved, and differentiation from seborrheic dermatitis is sometimes difficult (see Fig. 5.14 ). The diaper area is often spared (see Fig. 5.15 ). Prolonged AD with increasing discomfort disturbs sleep, and both the parents and the child are distraught.
). The scalp may be involved, and differentiation from seborrheic dermatitis is sometimes difficult (see Fig. 5.14 ). The diaper area is often spared (see Fig. 5.15 ). Prolonged AD with increasing discomfort disturbs sleep, and both the parents and the child are distraught.



For years, foods have been suspected as etiologic factors. Food testing and breast-feeding are discussed at the end of this chapter. The course of the disease may be influenced by events such as teething, respiratory tract infections, and adverse emotional stimuli. The disease is chronic, with periods of exacerbation and remission, and resolves in approximately 50% of infants by 18 months; other cases progress to the childhood phase, and a different pattern evolves.
Growth in Atopic Eczema.
Height is significantly correlated with the surface area of skin affected by eczema. The growth of children with eczema affecting less than 50% of the skin surface area appears to be normal, and impaired growth is confined to those with more extensive disease. Treatment with topical steroids has only a marginal additional effect on impaired growth.
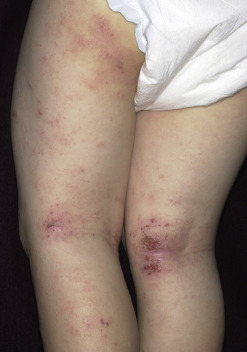
Childhood Phase (2 to 12 Years)
The most common and characteristic appearance of AD is inflammation in flexural areas (i.e., the antecubital fossae, neck, wrists, and ankles [ Figs. 5.16 to 5.20 ]). These areas of repeated flexion and extension perspire with exertion. The act of perspiration stimulates burning and intense itching and initiates the itch–scratch cycle. Tight clothing that traps heat about the neck or extremities further aggravates the problem. Inflammation typically begins in one of the fossae or around the neck. The rash may remain localized to one or two areas or progress to involve the neck, antecubital and popliteal fossae, wrists, and ankles. The eruption begins with papules that rapidly coalesce into plaques, which become lichenified when scratched. The plaques may be pale and mildly inflamed with little tendency to change (see Fig. 5.18 ); if they have been vigorously scratched, they may be bright red and scaling with erosions. The border may be sharp and well-defined, as it is in psoriasis, or poorly defined with papules extraneous to the lichenified areas. A few patients do not develop lichenification even with repeated scratching. The exudative lesions typical of the infant phase are not as common. Most patients with chronic lesions tolerate their disease and sleep well.








Constant scratching may lead to destruction of melanocytes, resulting in areas of hypopigmentation that become more obvious when the inflammation subsides. These hypopigmented areas fade with time ( Fig. 5.21 ). Additional exacerbating factors such as heat, cold, dry air, or emotional stress may lead to extension of inflammation beyond the confines of the crease areas ( Figs. 5.22 to 5.25 ). The inflammation becomes incapacitating. Normal duration of sleep cannot be maintained, and school, work, or job performance deteriorates; these people are miserable. They discover that standing in a hot shower gives considerable temporary relief, but further progression is inevitable with the drying effect produced by repeated wetting and drying. In the more advanced cases, hospitalization is required. Most patients with this pattern of inflammation are in remission by age 30, but in a few patients the disease becomes chronic or improves only to relapse during a change of season or at some other period of transition. Then dermatitis becomes a lifelong ordeal.
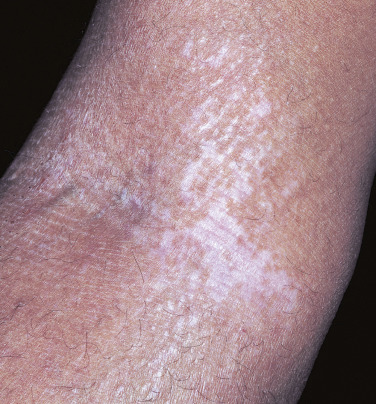






Adult Phase (12 Years to Adult)
The adult phase of AD begins near the onset of puberty. The reason for the resurgence of inflammation at this time is not understood, but it may be related to hormonal changes or to the stress of early adolescence. Adults may have no history of dermatitis in earlier years, but this is unusual. As in the childhood phase, localized inflammation with lichenification is the most common pattern. One area or several areas may be involved, and there are several characteristic patterns. Pigmentary alterations, especially hypopigmentation ( Fig. 5.26 ), may be seen and are distressing to patients.

Inflammation in Flexural Areas.
This pattern is commonly seen and is identical to childhood flexural inflammation.
Hand Dermatitis.
Hand dermatitis may be the most common expression of the atopic diathesis in the adult (see Atopic Hand Dermatitis in Chapter 3 ). Adults are exposed to a variety of irritating chemicals in the home and at work, and they wash more frequently than do children. Irritation causes redness and scaling on the dorsal aspect of the hand or around the fingers. Itching develops, and the inevitable scratching results in lichenification or oozing and crusting. A few or all of the fingertip pads may be involved. They may be dry and chronically peeling or red and fissured. The eruption may be painful, chronic, and resistant to treatment. Psoriasis may have an identical presentation.
Inflammation Around Eyes.
The lids are thin, frequently exposed to irritants, and easily traumatized by scratching. Many adults with AD have inflammation localized to the upper lids ( Fig. 5.27 ). They may claim to be allergic to something, but elimination of suspected allergens may not solve the problem. Habitual rubbing of the inflamed lids with the back of the hand is typical. If an attempt to control inflammation fails, then patch testing should be considered to eliminate allergic contact dermatitis.

Lichenification of the Anogenital Area.
Lichenification of the anogenital area is probably more common in patients with AD than in others. Intertriginous areas that are warm and moist can become irritated and itch. Lichenification of the vulva (see Fig. 3.53 ), scrotum (see Fig. 3.55 ), and rectum (see Fig. 3.54 ![]() ) may develop with habitual scratching. These areas are resistant to treatment, and inflammation may last for years. The patient may delay visiting a physician because of modesty, and the untreated lichenified plaques become very thick. Emotional factors should also be considered with this isolated phenomenon.
) may develop with habitual scratching. These areas are resistant to treatment, and inflammation may last for years. The patient may delay visiting a physician because of modesty, and the untreated lichenified plaques become very thick. Emotional factors should also be considered with this isolated phenomenon.
Associated Features
Dry Skin and Xerosis
Dry skin is an important feature of the atopic state. It is commonly assumed that patients with AD have inherited dry skin. The dryness may, however, reflect mild eczematous changes, concomitant ichthyosis, or a complex of both of these changes.
Dry skin may appear at any age, and it is not unusual for infants to have dry, scaling skin on the lower legs. Dry skin is sensitive, easily irritated by external stimuli, and, more importantly, itchy. It is the itching that provides the basis for the development of the various patterns of AD. Scratched itchy skin develops eczema; in other words, it is the itch that rashes.
Dry skin is most often located on the extensor surfaces of the legs and arms, but in susceptible individuals it may involve the entire cutaneous surface. Dryness is worse in the winter when humidity is low. Water is lost from the outermost layer of the skin. The skin becomes drier as the winter continues, and scaling skin becomes cracked and fissured. Dry areas that are repeatedly washed reach a point at which the epidermal barrier can no longer maintain its integrity; erythema and eczema occur. Frequent washing and drying may produce redness with horizontal linear splits, particularly on the lower legs of the elderly, giving a cracked or crazed porcelain appearance (see Chapter 3 , Fig. 3.43, Fig. 3.44, Fig. 3.45 ![]() ). Avoid frequent washing. Use mild soaps (e.g., Dove, Cetaphil bar) and routinely apply moisturizing creams or lotions. Moisturizers are effectively bound in the skin if they are applied shortly after patting the skin dry following bathing.
). Avoid frequent washing. Use mild soaps (e.g., Dove, Cetaphil bar) and routinely apply moisturizing creams or lotions. Moisturizers are effectively bound in the skin if they are applied shortly after patting the skin dry following bathing.
Ichthyosis Vulgaris
Ichthyosis is a disorder of keratinization characterized by the development of dry, rectangular scales. There are many forms of ichthyosis. Dominant ichthyosis vulgaris may occur as a distinct entity, or it may be found in patients with AD. Atopic patients with ichthyosis vulgaris often have keratosis pilaris and hyperlinear, exaggerated palm creases. Infants may show only dry, scaling skin during the winter, but with age the changes become more extensive, and small, fine, white translucent scales appear on the extensor aspects of the arms and legs ( Fig. 5.28 ). These scales are smaller and lighter in color than the large, brown polygonal scales of X-linked ichthyosis, which occurs exclusively in males ( Fig. 5.29 ). The scaling of the dominant form does not encroach on the axillae and fossae, as is seen in X-linked ichthyosis. Scaling rarely involves the entire cutaneous surface. The condition tends to improve with age. Application of 12% ammonium lactate lotion or cream or urea cream is very effective.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


