Upper Thigh Lift
Michele A. Shermak
DEFINITION
Upper thigh lift describes excision of lax and/or redundant thigh tissue to improve tautness, circumference, and/or shape of the thighs.
This procedure is often included in approaching lower body lifting for individuals who have sustained massive weight loss.
The procedure may be performed in combination with lifts of adjacent body regions such as the abdomen or back to globally improve the lower body region.
ANATOMY
Anatomic details of the thigh are shown in FIG 1.
The skin can demonstrate varying degrees of redundancy, vertical excess, laxity, and collagen strength. Thin skin may have greater recoil after surgery resulting in exacerbated loosening of the surgical result. Attention should be focused on the presence of varicose veins, and if there are many, referral to a vascular surgeon is prudent to minimize varicosities prior to embarking on thigh lift.
Subcutaneous fat varies in thickness.
A thinner fat layer is more appropriate for thigh lift than a thick one, which would more optimally lead to a liposuction contouring procedure or recommendation for weight loss.
The fat between the anterior thigh and posterior thigh is different: anterior thigh fat is thinner and softer, whereas posterior fat tends to be thicker and fibrous.
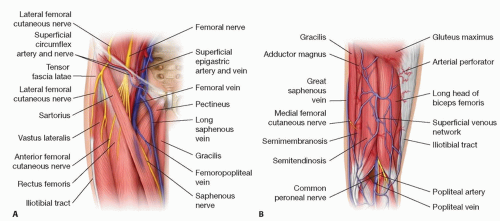
FIG 1 • A,B. Thigh anatomy is notable anteriorly for the saphenofemoral junction at the groin and the lymphatic collections at the groin and knee. External anatomy—skin quality, fat quantity, and superficial vein and varicosities—is variable in presentation.
The final scar appearance may be impaired by the difference in fat characteristics in the medial anterior and posterior thigh with fullness and visibility, particularly if posterior fat is pulled anteriorly.
Liposuction of the fat to be excised has been described to aid in better visualizing veins and lymphatics; however, liposuction may impair healing, and less is more may be the case here, with improved healing without liposuction performed in the area to be resected.
Scarpa fascia is the pseudofascial plane in the subcutaneous fat that is located superior to the greater saphenous vein on the inner thigh. The depth of this fascial plane is short in the groin area where penetration can lead to potential injury of the saphenofemoral veins and femoral artery or nerve.
Deep muscular fascia should be obscured by soft tissue with tissue undermining during thigh lift to help preserve the greater saphenous vein and lymphatics.
Muscles in this should not be visualized as the muscular fascia is not penetrated; surgery only involves the skin and subcutaneous fat of the inner thigh.
Patients seeking thigh lift may have superficial dilated varicose veins. The greater saphenous vein is important, because it is within the field of the vertical inner thigh lift and should not be traumatized, as injury may lead to distal extremity swelling. Perforators off the vein are ligated and cut. The saphenofemoral junction is close to the skin surface and may be seen and should be preserved.
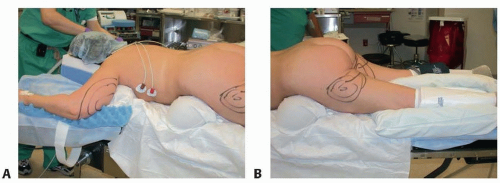
FIG 2 • Prone positioning helps provide the best access to the posterior thigh, when performing APEX proximal thigh lift. Safety measures while the patient is in prone position include the following: A. Face in prone pillow with goggles protecting eyes from pressure and desiccation; arms are placed at 90 degrees, and gel bumps are placed under the chest and lumbar region. B. Bump under chest lumbar regions and forced warming blanket to avoid hypothermia.
Dissected thigh tissue is always discarded, so arterial perforators are ligated and cauterized, and no major arteries are within the field of dissection. The femoral artery is close to the skin surface, and dissection should be carefully performed in the groin.
Dissection deep to superficial fascia may result in injury to lymphatics, which travel close to the saphenous vein. Lymphoceles may develop postoperatively near the knee where lymphatics are dense.
PATHOGENESIS
With skin laxity and/or weight loss of varying degrees, individuals can suffer from excess skin in the thigh.
This may be focally limited to the proximal aspect of the inner thigh with minimal skin change outside of this area, most often seen in younger massive weight loss patients.
On the other hand, others present with more diffuse, global changes in the inner thigh, with significant attenuation and redundancy of the skin, typically in the older, thinner patient who has experienced massive weight loss.
A more extended approach to thigh lift in this patient population will reduce circumference and improve skin appearance all the way to the knee.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patient history should be probed for significant weight loss and, if present in the history, the mode and degree of weight loss, as well as nutritional challenges that may exist.
Weight should be stable at the time of surgery at least 3 months.
Medical conditions that may impact outcome of thigh lift surgery such as peripheral vascular disease, varicose veins, venous thromboembolism, diabetes, heart disease, sleep apnea, autoimmune and endocrinological disorders, and coagulation disorders and venous thromboembolic history should be queried.
Any history of surgery in the groin region must also be addressed, such as that performed for lymph node biopsy.
Physical findings should note skin quality and degree of excess and redundancy and varicosities as well as adiposity.
Chronic calf swelling needs to be noted if present.
Adjacent body regions such as the mons pubis, abdomen, and back are examined to see if addressing these regions will improve overall lower body aesthetics.
SURGICAL MANAGEMENT
Preoperative Planning
Preoperative planning with thigh lift includes addressing significant varicose veins ahead of surgery, as well as discussion of different thigh lift approaches with differing scar lengths.
More focal proximal skin excess and good skin quality lend themselves well to proximal scar along groin crease, which is well hidden.
More extended involvement to the knee with attenuated skin and cellulite may be better addressed with vertical incision along the length of the inner thigh.
With existing calf swelling, the more limited proximal approach is preferable as the more extended thigh lift approach can exacerbate thigh swelling.
Widened mons pubis may be treated at the time of thigh lift, with inclusion of lateral mons tissue within the zone of resection, paired with liposuction of the mons, as needed (see Chapter 19).
Positioning
Positioning varies depending on the thigh lift approach.
The proximal approach requires prone to supine positioning to treat posterior dog-ear and impact of result by extending excision into the infragluteal fold.
Prone positioning precautions must be followed in the head and neck area and upper body, as well as the gluteal region and thighs.
Gel rolls are placed along the upper chest/axilla, and the neck is placed in a neutral position with head resting in prone pillow and eyes off-loaded.
Arms at elbow and axilla placed at no greater than 90 degrees with padding under arms and legs to protect pressure points (FIG 2).
The more extended vertical inner thigh excision requires only supine positioning.
In the supine position, thigh lift is most easily performed with leg extension bars off the end of the operating room table to allow the surgeon to stand or sit between the legs, which are spread apart from each other.
Positioning of the thighs in stirrups as seen in gynecological surgical procedures is not necessary and puts the patient at risk for venous thromboembolism (VTE) at the groin with flexion of the hip.
Approach
Direct excision of the skin excess of the inner thigh is performed.
Approach must be symmetrical and may include lateral mons pubis to reduce the pubis, which may be widened and full.
Excision at the lower aspect of the pubis in the groin is most at risk for high tension, so a bottleneck in the excision is created at this point to avoid too much tension and predilection for wound healing problems or pull on the mons pubis or labia.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








