Tissue Expansion for Trunk Defects
Ibrahim Khansa
Jeffrey E. Janis
DEFINITION
Tissue expansion is the mechanical increase of the surface area of tissue. It relies on two phenomena:
Creep: deformation of the tissue in response to stress
Stress relaxation: gradual decrease in the amount of force required to stretch the tissue over time
ANATOMY
In the trunk, the tissues most commonly expanded for wound coverage are the skin and subcutaneous tissue.
PATHOGENESIS
As the skin and subcutaneous tissue are expanded, all layers get thinner, except for the epidermis, which undergoes cellular hyperplasia via mitosis.1
After removal of the tissue expander, all layers return to normal thickness, except the adipose layer, which permanently thins.
Expanded skin has improved vascularity compared to nonexpanded skin.
Around the tissue expander, a capsule forms, consisting of collagen and fibroblasts. The zone between the native tissue and the capsule is highly vascular.
PATIENT HISTORY AND PHYSICAL FINDINGS
Tissue expansion is indicated when there is a local deficiency of soft tissue coverage over a wound, with healthy tissue in the surrounding zone that is able to be expanded.
Ask about history of radiation, because this makes radiated tissues much more stiff and difficult to expand and increases the risk of tissue expander exposure, infection, and/or loss.
On physical examination, look for infection/contamination, as this increases risk of complications with tissue expansion.
In the lower abdominal wall, regional transfer of tissues from the anterolateral thigh may be a better option for soft tissue coverage than tissue expansion. However, in the epigastric region, those flaps may not have sufficient reach. In addition, the epigastric region often has a scarcity of soft tissue, which increases the usefulness of tissue expansion in this area.
IMAGING
No imaging is required specifically for tissue expansion.
SURGICAL MANAGEMENT
Preoperative Planning
Control contamination
Mupirocin nasal ointment and chlorhexidine baths for 5 days preoperatively in patients at risk for methicillinresistant Staphylococcus aureus (MRSA) or who are known MRSA carriers.
This protocol has been shown to reduce surgical site infections in total joint arthroplasties.2
Optimize the patient to lower complication rates:
Glucose control: Hemoglobin A1c should be ≤7.4%.3
Obesity: BMI should be 42 or lower and preferably below 40.3
Tobacco usage: Patients should quit all tobacco products for 4 weeks preoperatively and 4 weeks postoperatively.3
Tissue expander selection
Choose largest tissue expander that can be placed in the pocket.
Length of the expander should be at least as long as the defect.
Crescentic and rectangular tissue expanders tend to be best suited for abdominal wall defects. Rectangular expanders tend to have the highest yield.5
Remote port tissue expanders are preferred.
Positioning
Supine with arms abducted 90 degrees, with all pressure points padded
Approach
The planned flap movement should be designed before tissue expansion is begun. The incision to insert a tissue expander is usually made very close to the border of the soft tissue defect. This helps minimize the amount of tissue between the leading border of the flap and the wound, which will be discarded, and provide for expansion of uninjured/unscarred tissue to transpose later directly to the defect.
TECHNIQUES
▪ Subcutaneous Tissue Expander Insertion Into the Abdomen
Prep the skin with alcohol-containing prep (chlorhexidine and alcohol or iodine and alcohol).3,6 If a wound is present, use iodine alone.
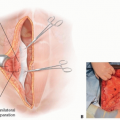
Design an advancement or rotation flap, which, when expanded, will cover the defect. The leading edge of the flap should be along one of the edges of the defect (TECH FIG 1A).
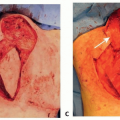
Make an incision within 3 to 5 mm of the edge of the defect. This will serve as the insertion access for the tissue expander and the leading edge of the flap. The incision should not be made immediately at the edge of the wound, as this incision will need to be closed and requires healthy tissue to obtain a closure robust enough to protect the tissue expander (see TECH FIG 1A,D). However, minimize the amount of tissue between the edge of the wound and the incision, as this tissue will be discarded.
Dissect down to the anterior rectus sheath, and elevate the skin and subcutaneous tissue off the rectus sheath from medial to lateral. The length and width of the undermining should correspond precisely to the dimensions of the tissue expander (TECH FIG 1B).
Once the precise pocket is dissected, create an additional small pocket for the remote port. Through the dissected expander pocket, choose a location for the remote port adjacent to the expander. The location should be chosen so that the remote port is distant enough from the expander to avoid expander puncture during fills, where the subcutaneous tissue is thinnest in order to facilitate palpation of the port during fills, and preferably over a bony area to provide support during needle access/insertion during fills. Dissect a small pocket that will precisely fit the remote port. Do not overdissect, as this could result in port migration or rotation.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree