For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
Introduction
The human mind instinctively examines another’s eyes before any other facial feature. Trustworthiness, aggression, and even fertility are conveyed by the appearance of the eyes. The periorbital region influences facial harmony and is the most powerful tool for nonverbal communication and expression. For these reasons, esthetic enhancement of the upper eyelid has been sought after for centuries and is one of the most commonly performed cosmetic operations today.
Patients seek correction of excess skin, tired or sad-looking eyes, and droopy eyelids, which can often be achieved with upper blepharoplasty. Other rejuvenation techniques, including brow and midface lift, skin resurfacing, and volume restoration with fat or dermal fillers may also be utilized. Upper eyelid blepharoplasty is often perceived as technically simple with high reward and relatively low risk. This can subsequently translate to surgeon complacency and universal application of the same techniques to all patients. An improved understanding of periorbital aging and evolving patient expectations have led to the development of more effective surgical approaches in upper blepharoplasty.
Periorbital Aging
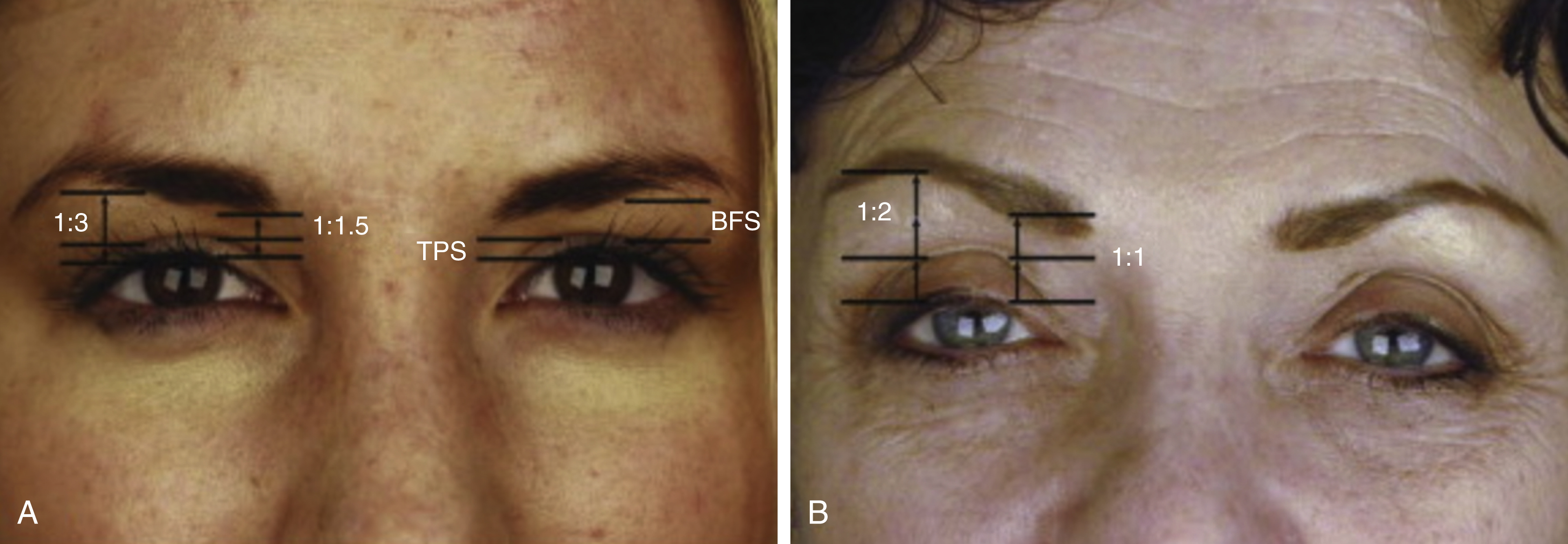
Aged appearance of the upper lid is influenced by skin quality, volume of the eyelid and position of the brow and periorbita. The youthful upper eyelid is voluminous and smooth with a crisp upper lid crease. The relationship of the brow to the upper eyelid has been described by Goldgerg and is emphasized when examining the esthetics of the periorbital region. The term brow fat span (BFS) represents the distance between the brow and upper lid crease; tarsal platform show (TPS) is the distance from the lid crease to the upper eyelid margin. Studies have identified that a youthful TPS:BFS ratio is 1:1.5 medially and 1:3 laterally ( Fig. 64.1 ).
Signs of aging result from environmental factors including sun exposure and smoking but also from genetic characteristics such as familial fat pseudoherniation which may be apparent in the teen years. With age, patients experience soft tissue ptosis and loss of orbital bony support. Dermatochalasis is caused by loss of skin elasticity. Thinning of the orbicularis oculi and weakening of the orbital septum lead to pseudoherination of orbital fat resulting in a heavy appearance to the upper lid. Hooding of the lid is caused by atrophy of temple, brow, and eyelid fat. Brow ptosis is more significantly impacted by volume loss rather than actual decent of the brow.
Anatomy
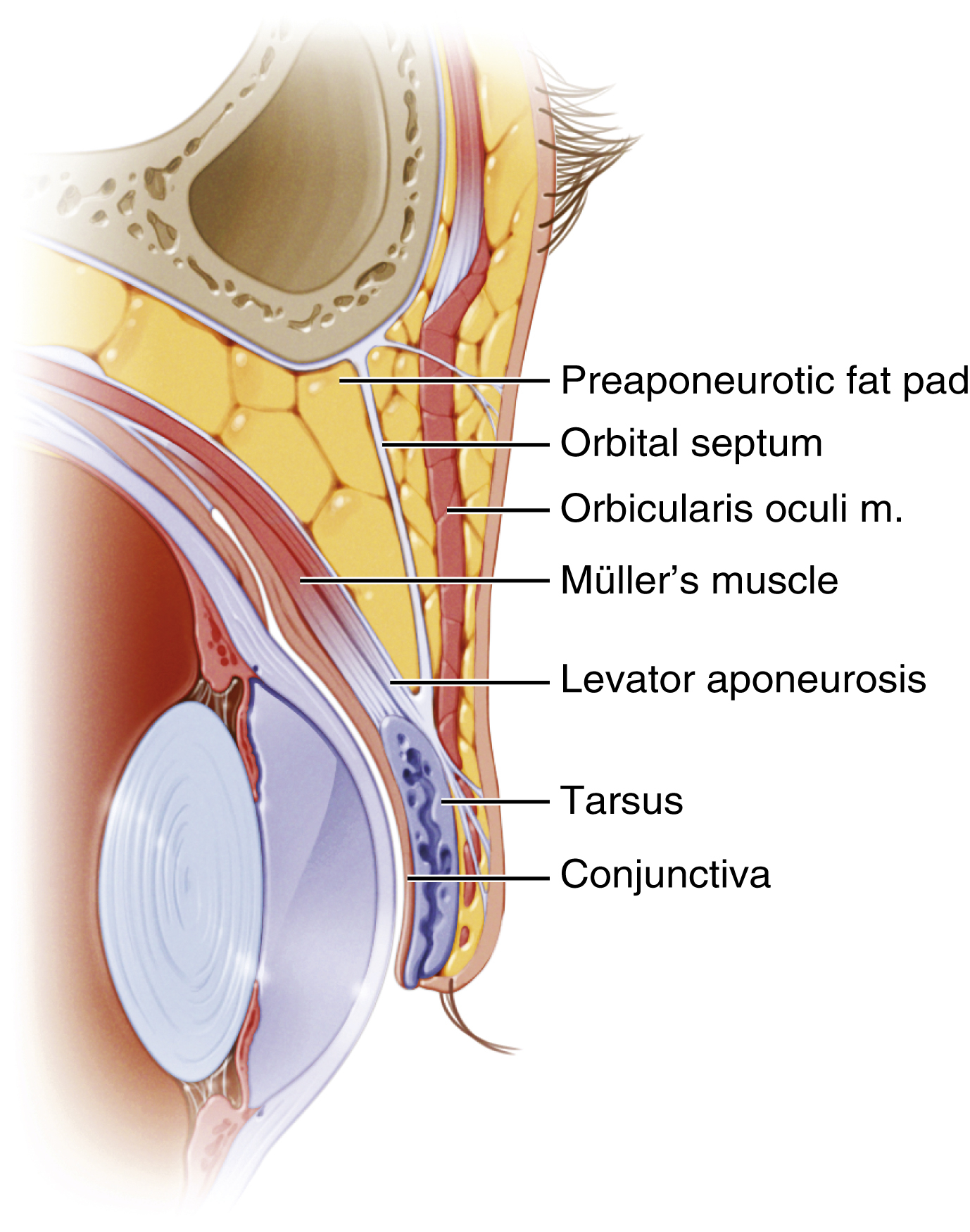
The upper eyelid is composed of anterior and posterior lamellae. From superficial to deep, the layers include: skin and orbicularis oculi muscle (which make up the anterior lamella), retro-orbicularis oculi fat (ROOF), orbital septum, orbital fat, levator palpebrae muscle superiorly and levator aponeurosis inferiorly, Müller’s muscle inserting to tarsal plate and conjunctiva (the latter two forming the posterior lamella) ( Fig. 64.2 ).
The upper lid skin is the thinnest in the body and is intimately associated with the underlying orbicularis oculi muscle. The orbicularis oculi contains voluntary and involuntary muscle and is innervated by the temporal branch of the facial nerve. It is composed of orbital, preseptal, and pretarsal components, named for the underlying structures. Pretarsal orbicularis oculi forms the medial and lateral canthal tendons.
The orbital septum is an extension of orbital periosteum and originates at the arcus marginalis. It separates eyelid (preseptal) from orbital (postseptal) contents and confines the orbital fat. The upper eyelid contains two fat compartments, one medial and one central, which are separated by the trochlea. The lacrimal gland lies laterally in the same plane as the orbital fat and appears pink and firm, compared to the soft yellow fat compartments.
The levator muscle is located deep to the orbital fat and is the major retractor of the lid. The upper lid crease is formed by the insertion of the levator aponeurosis and orbital septum into the orbicularis oculi and skin. The lid crease is 7–9 mm superior to the lid margin in women and 5–7 mm in men. In the occidental eyelid, this fusion occurs superior to the tarsal border. In the Asian eyelid, the levator aponeurosis and orbital septum attach further inferiorly and anterior to the tarsus. This creates fullness of the upper lid and prevents crease formation ( Fig. 64.3 ). Whitnall’s ligament is formed by a thickening of the levator aponeurosis and suspends the levator muscle from the trochlea to the lacrimal gland fossa. Müller’s muscle arises from the undersurface of the levator aponeurosis and attaches to the superior tarsal plate. It has sympathetic innervation and produces 2–3 mm of eyelid retraction.

Patient Evaluation
As with any cosmetic procedure, diligent patient evaluation and selection in upper blepharoplasty is critical to successful outcomes. Preoperative documentation should include full medical history, medications, and dedicated ophthalmological history. Specifically, the patient is questioned regarding vision, use of corrective lenses, esthetic concerns, symptoms of dry eye or excess tearing, history of ocular disease (trauma, glaucoma, Grave’s ophthalmopathy), and previous facial surgeries. Upper blepharoplasty should be delayed at least 6 months following refractive corneal surgery.
The examination begins with obtaining standard preoperative photographs including:
- •
Full face frontal, oblique, lateral
- •
Close-up frontal with eyes in neutral gaze, upward gaze, and eyes closed
- •
Close-up lateral and oblique of each eye.
The patient is then examined in a sitting position and facial repose. When determining candidacy for upper eyelid surgery, specific anatomical and physiological factors should be evaluated. They include:
- •
Skin elasticity and texture
- •
Frontal and temporal hairline position
- •
Eyebrow shape, position, mobility, texture, and symmetry
- •
Position may be influenced by involuntary contraction of the frontalis muscle in patients with lateral hooding. To eliminate this, patients should close their eyes and the surgeon stabilizes the brow as the eyes are opened
- •
- •
Forehead and lateral canthal (crow’s feet) rhytids
- •
Deep set orbits or upper lid hollowing
- •
Upper lid dermatochalasis, tone, hooding and presence of herniated fat pads
- •
Evidence of prior surgery or scarring
- •
Presence of lagophthalmos (inability to close the palpebral fissure completely) and ptosis
Visual acuity and visual field testing should be performed, especially if there are functional concerns. Severity of dry eye can be assessed with Schirmer’s test and patients should be counseled that upper blepharoplasty may worsen symptoms of dry eye.
The patient’s expectations and motivations for seeking plastic surgery must also be carefully analyzed and discussed during the initial consultation. Patient dissatisfaction frequently arises secondary to poor communication regarding the surgical goals and unrealistic patient expectations. A patient seeking a blepharoplasty who is found to have significant brow ptosis and little dermatochalasis should be counseled that a brow lift may be the best option. It is the responsibility of the surgeon to guide the patient toward the approach that will best address their concerns. Following the education process, candidates for upper eyelid rejuvenation must give informed consent after the possible adverse outcomes and risks of the selected surgical procedure are discussed.
Surgical Techniques
Generally, brow elevation procedures are performed prior to upper blepharoplasty to allow for the appropriate amount of upper eyelid skin to be removed. This helps to prevent excessive elevation of the brow–lid complex and subsequent lagophthalmos.
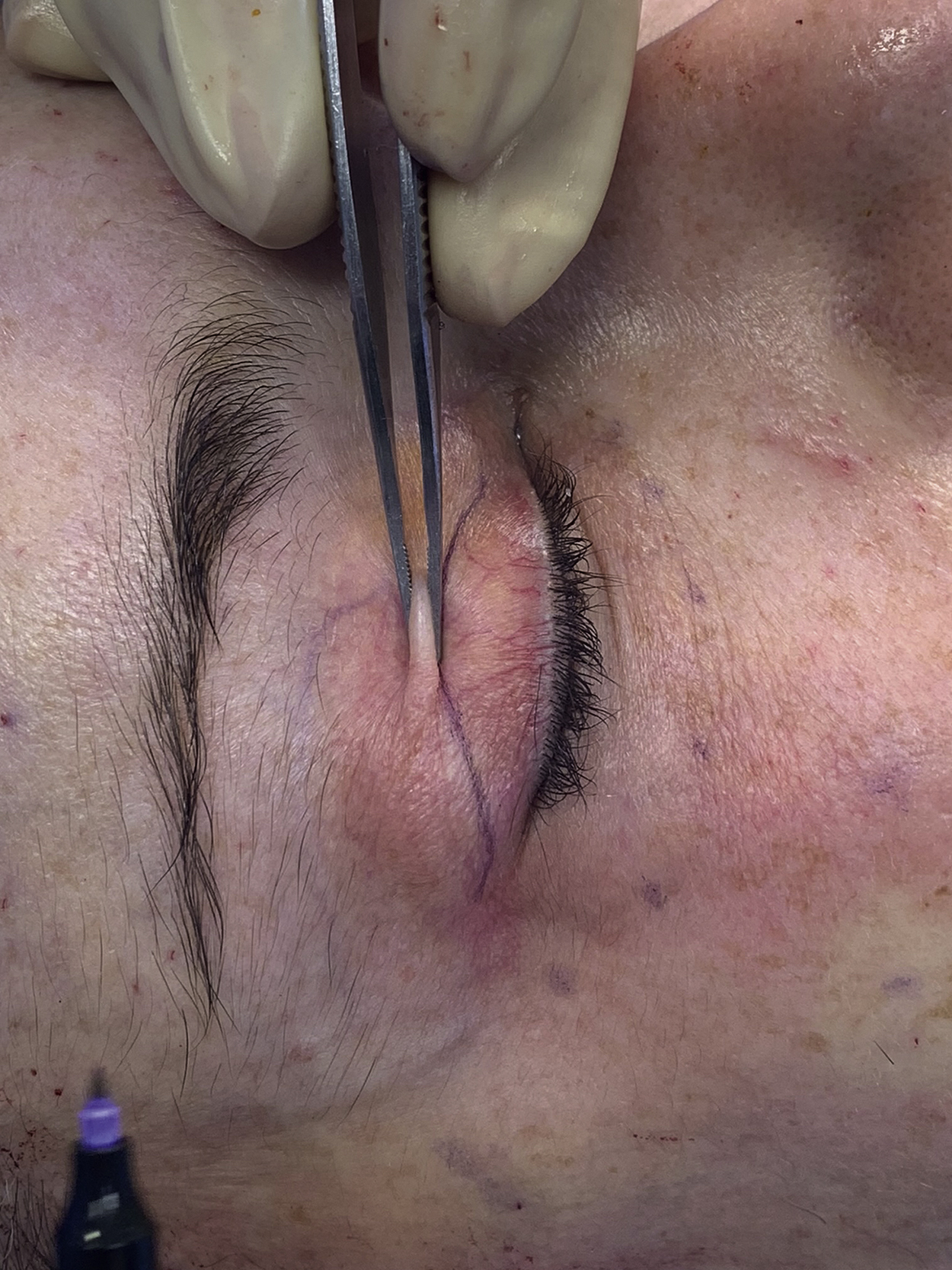
Marking
Many surgeons prefer marking of the upper lid to be done with the patient in a seated position, however it is the practice of the authors to mark the patient while supine. The natural upper lid crease is marked as the inferior limb of the incision, approximately 6–9 mm above the lid margin. A caliper is used, and exact measurements are recorded. It is imperative to mark the skin with a fine-tip marking pen with the lid skin under tension. The amount of skin to be excised is estimated with a pinch technique ( Fig. 64.4 ). The lateral marking is curved superiorly and should not extend lateral to an imaginary line drawn from the lateral canthus to the tail of the brow ( Fig. 64.5 ). More skin is taken laterally to address lateral hooding. It is important to maintain a minimum of 20 mm of lid height to guarantee normal lid closure. The superior marking should be at least 10 mm from the inferior border of the brow to maintain an appropriate brow–fat span distance. Fat pseudoherniation is also identified and marked preoperatively.