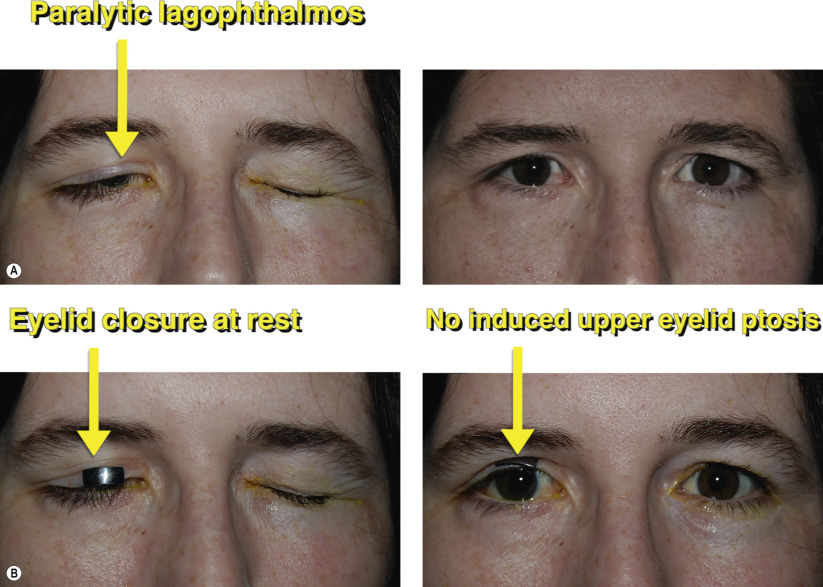
| Paralytic lagophthalmos |
| Exposure keratopathy |
| CN VII palsy |
| Symptomatic dry eye |
| Bell’s phenomenon |
| Degree of lagophthalmos |
| Corneal epithelial staining |
| Orbicularis strength |
| Anterior or posterior lamellar shortage |
| Prior eyelid, facial surgery or trauma |
| Corneal sensation |
| Office testing of external weight loading to determine appropriate size |
Introduction
Adequate closure of the eyelid is essential to maintain clarity and comfort of the ocular surface. This includes a normal blink as well as complete closure during rest. Patients with adequate lubrication and a good Bell’s phenomenon can tolerate some degree of lagophthalmos in maintaining ocular surface integrity.
Patients with uncompensated lagophthalmos may develop ocular symptoms of pain, foreign body sensation, and dryness. Their cornea may show signs of punctate epithelial defects. An assessment of corneal sensation should be made as these patients may develop rapid corneal decompensation and even perforation. Idiopathic facial nerve palsy should first be managed medically for spontaneous resolution unless corneal compromise occurs. In contrast, other patients may have permanent facial nerve palsy, i.e., after removal of parotid gland tumors where no recovery of nerve function is expected.
If maximal medical therapy with ocular lubricants and eyelid occlusion fails, patients with symptomatic dry eye and corneal findings may be candidates for eyelid loading. An external load can be placed to determine the appropriate weight. The lightest load to allow complete closure is the goal without inducement of ptosis. External weights for daily use are available with double stick adhesive (MedDev, Palo Alto, CA) if the patient wishes to experience eyelid loading prior to implantation ( Figures 19.1A and 19.1B )
Different techniques of placement and choices of weight exist. Platinum is a suitable choice as a weight for eyelid loading. Compared to gold, the same platinum weight has a thinner profile owing to its lower molecular weight. Furthermore, certain patients have an allergy to gold (or to nickel, a common element that is used in production). While some surgeons have advocated more superior implantation, above the tarsus beneath the levator, our preference is for tarsal fixation within a relatively superior pretarsal pocket. The weight is secured through the pre-existing holes directly to the tarsal plate. It is important to perform layered closure with the orbicularis to prevent exposure. A small graft of temporalis fascia may also be used if tissues are thinned and atrophic. In long-standing cases of paralytic lagophthalmos, unopposed levator action for many years may have caused some contraction and a levator recession may be necessary to allow the eyelid to close ( Chapter 17 ).
If a properly selected weight is determined during the preoperative examination, the eyelid load should be adequate to close the eyelid at rest. Patients may need to be aware to more consciously allow eyelid closure from gravity, as there may be some momentary time lag. If the eyelid load is too light or too heavy, it may be easily removed and replaced. In cases where facial nerve function returns, the weight may be explanted.
Preoperative Evaluation