Given the central importance of the “eyes,” meaning the periorbital region, to facial appearance, the motivated blepharoplasty patient has the opportunity to improve appearance significantly beyond the minimum of age reversal, to reveal inner beauty or add attractiveness. Bright and beautiful eyes have good three-dimensional contouring. The benefits of a quality eyelid crease enable the surgical focus to be on lid contouring with a reduced requirement for lid skin and fat excision. A durable crease maintains fixation of both the tarsal and infrabrow segments. The softness of youthful eyes can be regained by precise, but cautious, use of lipofilling.
Key points
- •
Because the “eyes” are of the highest importance in facial appearance and identity, it behooves the surgeon of the motivated patient to go beyond simple age reversal, to reveal inner beauty or add attractiveness.
- •
A nuanced understanding of facial aesthetics is required of the surgeon, along with refined surgical technique, which includes detailed intraoperative recognition of lid anatomy.
- •
A blepharoplasty technique based on a lid crease that is stable and lasting provides independent control of both lid segments. A major skin resection is avoided as is unnatural skin tension, visible scars, and the subsequent postblepharoplasty “look.”
- •
Simultaneous correction of the age-related diminution of the orbital rim fat volume adds a level of aesthetic refinement, while avoiding the “operated eye look.” Simultaneous correction of a deficient supraorbital rim projection enhances the result in those patients.
Video content accompanies this article at http://www.facialplastic.theclinics.com
Good is the enemy of best. —Mark Twain
This article represents the personal understanding of an individual plastic surgeon that evolved with a broad experience over the course of his career in aesthetic surgery of the face. It does not replace the “how to guide” for the learning surgeon, for whom much is well presented elsewhere. Rather the concepts may appeal to some individual surgeons, who find satisfaction in the possibilities of aesthetic surgery. All surgery requires quality of practice, but when a person’s face is involved, quality has a different significance. This is because of the personal and social impact that surgery of facial appearance has on that person’s identity and self-esteem, reflecting how other people are influenced by, and respond to the appearance, usually at a subconscious level.
This significance was succinctly described last century by Egon Brunswick (1934), a psychologist: “ a small change in facial proportion, changes our perception of a person’s personality ”.
This article is based around a refinement in perceptual understanding, then of the relevant anatomy, leading to the surgery required to obtain the intended result. There are several aspects involved in the aesthetics of the “eye” including illusion, something women know from their experience of using cosmetic eye makeup. Even the term “makeup” tells a story!
Upper lid blepharoplasty is the centerpiece in rejuvenation of the periorbital region and also in glamorization of the eyes. However, a blepharoplasty is part of a larger story. This is because attractive eyes have a strong 3-dimensional aspect to them. Beautiful eyes are in a “picture frame” formed by the bony orbital rim, which is highlighted by the brows ( Fig. 1 ).

The 3-dimensional contour begins with the relationship between the picture frame, the superior orbital rim, and the globe and continues with the relationship between the 2 parts of the lid ( Fig. 2 ). The upper part of the lid is the connection between the brow and the globe. Eye shadow is traditionally applied to glamourize the eyes by creating the illusion of a greater depth of the lid recess, which indicates its importance in Society.
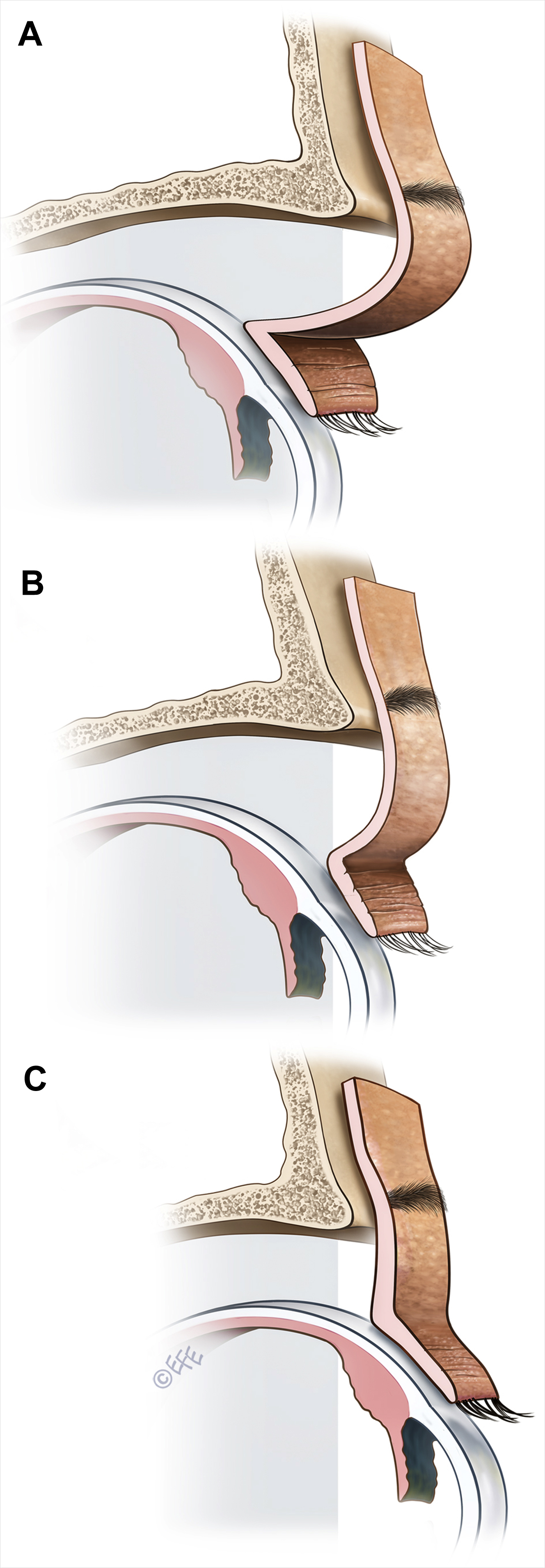
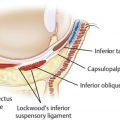
Although the lid is considered a single entity, it is structured of 2 segments that are anatomically separated by the lid crease ( Fig. 3 ). These are the lid proper, the lower part, the tarsal segment , and above that, the infrabrow segment . The lid fold is the lower part of the infrabrow segment that tends to hang over and conceal the lid crease to a varying degree. The lid fold varies considerably according to race, it may even be absent, and its variation over time is such that it ages a person. Hence, management of an excess lid fold is the usual surgery of upper lid blepharoplasty. Although interrelated, the 2 segments are visually and functionally separate. The hidden crease, with its function of internal fixation influences the appearance of the lid by balancing the 2 lid segments. Unfortunately, there is some confused terminology in some quarters; the terms “crease” and “fold” are confused as if they are the same thing. The crease is an inversion, which cannot be filled, and the fold is the opposite.
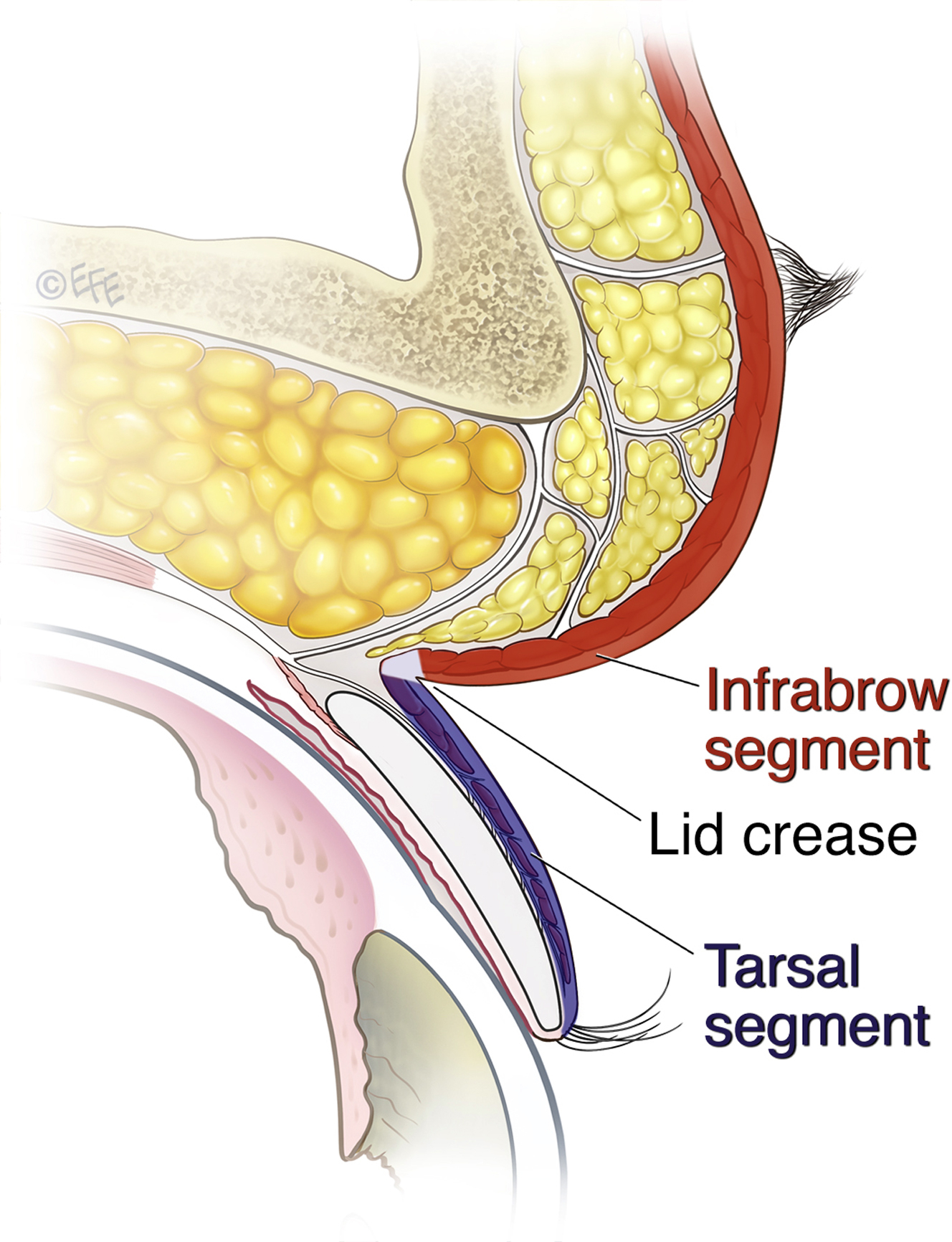
The tarsal segment moves across the upper globe as a unit, based on the fixed tarsal plate dimensions. Its moves as a unit. In contrast, the infrabrow segment is constantly changing its shape and dimensions, as it bridges the gap between the brow above and the mobile tarsal segment. The “look” of the eyes is most strongly determined by the lid show , the amount of the tarsal segment visible below the lid fold. Clearly the fold is under the influence of the infrabrow segment. It varies not only in its position but also in its quality. The well-defined surface appearance of an attractive lid reflects the internal anatomy ( Fig. 4 ).

Upper lid blepharoplasty
For more than 30 years the senior author has used, and refined, a tarsal fixation technique of upper lid blepharoplasty, first learnt from Dr Robert Flowers. This technique progressively replaced the use of the previously used standard excision technique because it provides the surgeon with precise control and predictable and extraordinarily lasting results. These benefits come at the price of a longer operating time and increased risk, both of which are reduced with experience involving a learning curve. The aesthetic, anatomic, and technical considerations are shared later, and the role of the brow is integral in the result.
Surgical control, paramount for quality surgery, is obtained in the technique by considering the 2 interconnected segments of the lid as separate and distinct. Each lid segment is appropriately corrected, independent of the other. The procedure is not difficult to master once the surgical steps are understood, although, the surgeon’s ability to recognize the internal anatomy is more critical than in traditional blepharoplasty.
Planning the tarsal segment is the first priority. The location of the marking for the lower incision (lower marking) is traditionally placed at a predetermined distance from the lid margin, correlating with the lowest skin crease. A logical alternative is to precisely locate the lower incision, whichis determined by the patient’s tarsal plate.
Surgical Technique
Preliminary markings
These are performed with the patient relaxed but cooperative. Three cardinal reference points are first marked on the lashline, with the patient looking at the same distant object. These are the medial limbus, medial pupil, and lateral limbus. Then the provisional lower marking is lightly placed.
The upper marking is made from the brow down, with the brow gently pushed down or naturally relaxed with the patient sitting.
The upper marking of the excision is challenging, as it requires judgment. It is located in reference to the patient’s brow position, being placed lower (less skin excision) if more skin needs to be retained due to inherently high and/or forward projecting brows. The usual distance is within the range, 17 to 21 mm, which according to standard excisional only blepharoplasty is not removing sufficient skin. More skin must be retained for the skin inversion of the tarsal fixation. This skin is “released” during lid closure, which prevents lagophthalmos.
Final markings
When the patient is deeply sedated or asleep, the lid is readily everted. Now, the shape of the patient’s tarsal plate is clearly seen and noted, then using the caliper, the maximum height of the tarsal plate (distance X) is measured ( Fig. 5 ).
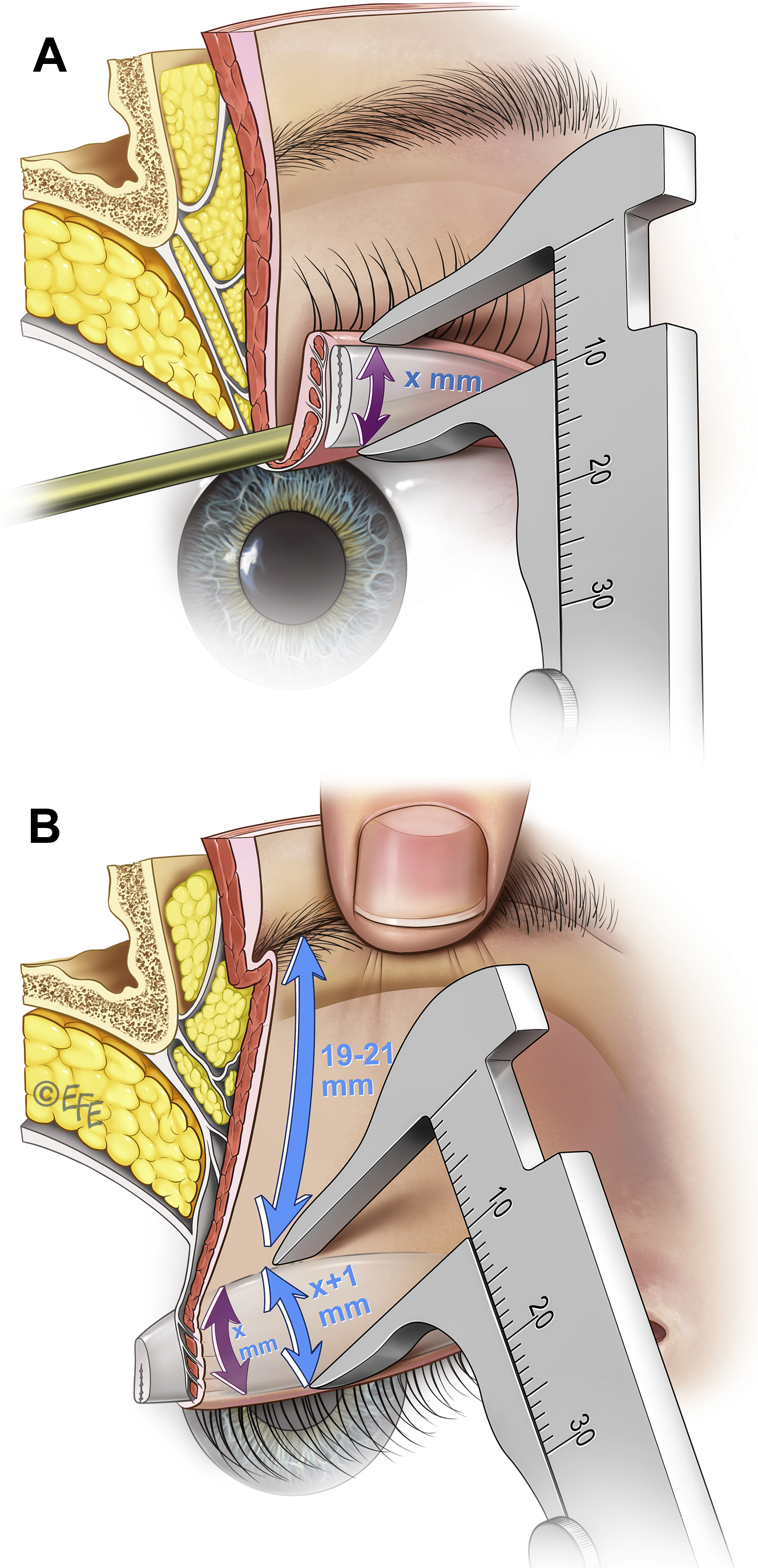
The position for the lower skin incision is calculated (X plus 1 mm) and this skin marking now made at the 3 cardinal points. As the marking is being performed, the skin should be placed under the natural tension intended for the final result.
Medial to the medial limbus up to the punctum, the marked distance is reduced to 7 to 8 mm. Similarly, over the lateral canthus the marking is about 8 mm, extending laterally as far as required to excise any moderate temporal hooding but significantly less than with a standard blepharoplasty due to the skin inversion inherent in the technique. The planned skin excision is confirmed by a pinch test and adjusted accordingly.
Excision of skin and muscle
Compared with a traditional blepharoplasty a considerably smaller amount of skin is resected as skin tension is to be avoided.
The skin only is incised, first along the lower incision, then the upper incision, and then carefully removed off the outer surface of the orbicularis with meticulous hemostasis on the muscle surface.
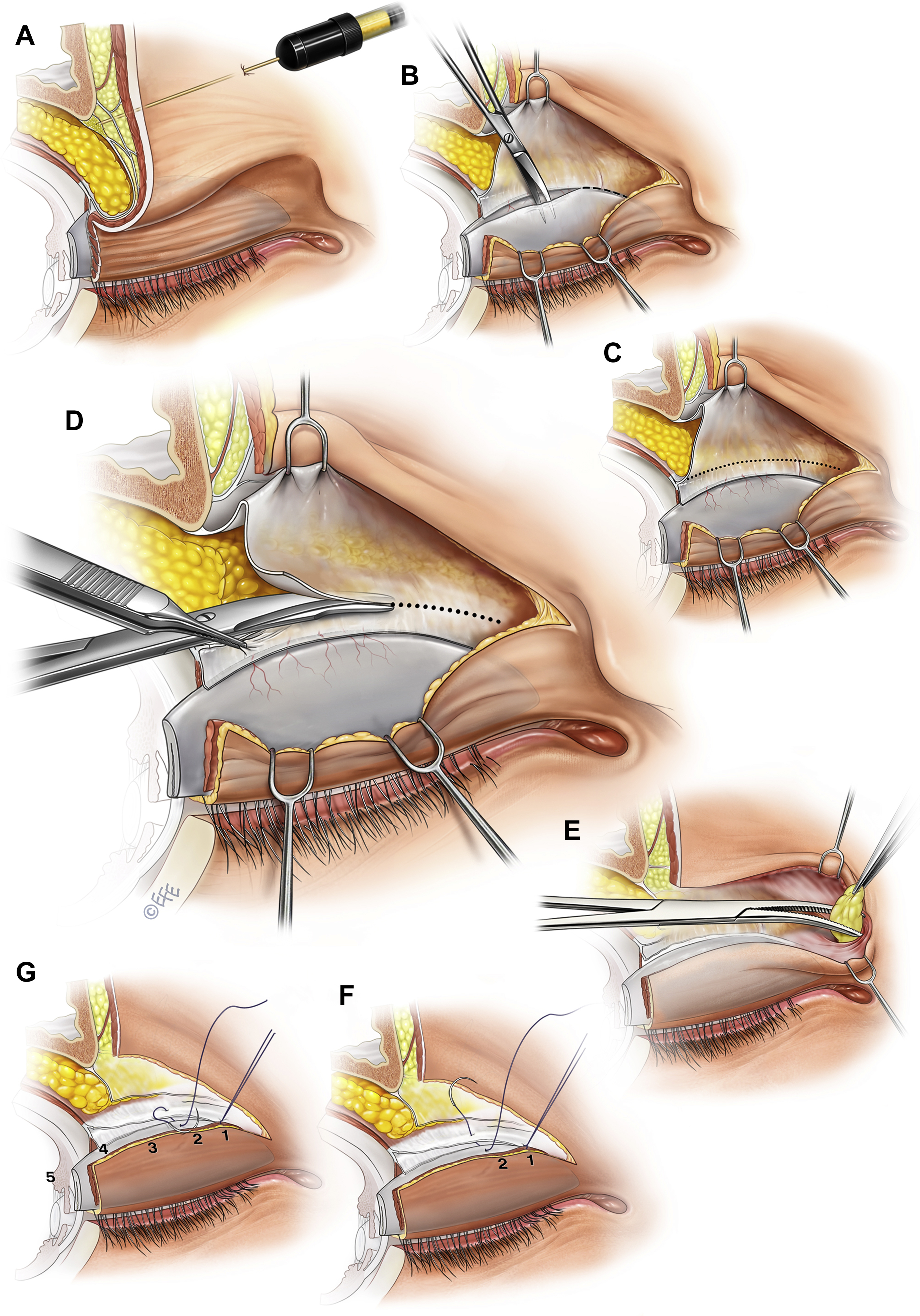
The orbicularis is then incised along the lower incision ( cutting diathermy or scalpel ), bevelling down slightly toward the upper border of the tarsal plate. Lateral to the lateral canthus a small strip of orbicularis is removed to avoid a dog ear at closure.
Defining the tarsal plate
The filmy areola tissue (the pretarsal extension of the levator) is then removed off the tarsal plate. To do this, the orbicularis is first elevated, then the areolar tissue carefully released from the underside of the orbicularis muscle fascia, continuing this dissection as far down toward the lashes as required, according to the pretarsal skin laxity. Both ends of the tarsal plate and the upper edge should be clearly defined. It is not necessary to routinely clean soft tissue off the lower edge of the levator, but if trimming is required, it must be done carefully to avoid shortening of the levator. The removal of the areolar tissue enables, what Dr Flowers described as, the underside of the orbicularis (its fascia) being “wallpapered” onto the tarsal plate surface.
Defining the Levator Edge
The septum orbitale is incised just above the sling , where it joins the levator. Identification of the levator is commenced at the lateral extent where it is safer from unintentional levator shortening.
Once it is confirmed that the scissor tip is on the surface of the levator with the septum orbitale, just superficial, a meticulously release of the septum off the levator is performed, continuing medially ( Fig. 6 C,D). Unintended shortening of the levator must be avoided, especially in the medial third where the edge of the levator is less distinct.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


