CHAPTER 9 Upper Blepharoplasty in the Asian Patient
Because the anatomy of the Asian eyelid differs from that of the Caucasian eyelid, I believe that a separate chapter emphasizing the difference is important. In the first edition, I showed how to westernize, or occidentalize, the Asian appearance by constructing an eyelid crease similar to the technique used in Caucasians. It later became apparent that most Asians would like to enhance their appearance by having a crease that conforms with Asian features, and this chapter was added.
Anatomy
Upper eyelids
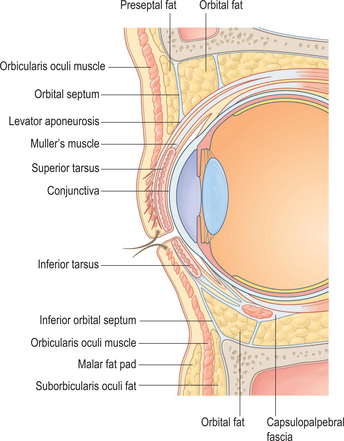
The difference between the Asian and Caucasian eyelid lies at the lower point of fusion of the orbital septum with the levator aponeurosis.1 In Caucasians (Fig. 9-1), the orbital septum fuses with the levator aponeurosis at approximately 8–10 mm above the superior tarsal border, limiting the downward extent of the preapo-neurotic fat pads while allowing the terminal inter-digitations of the aponeurosis to insert toward the subdermal surface of the pretarsal upper eyelid skin, starting along the superior tarsal border and heading inferiorly. As a result, when the levator muscle contracts and pulls the upper eyelid up, the skin forms a crease above the superior tarsal border and the skin above the crease forms the fold.
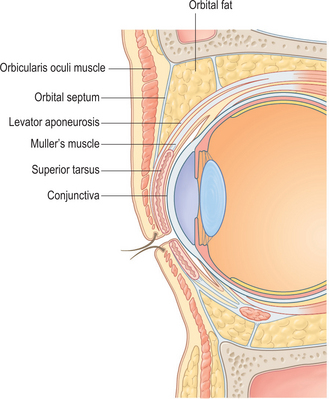
In Asians who do not have this crease (Fig. 9-2), as suggested by the anatomic studies of Doxanas and Anderson,1 the point of attachment of the orbital septum to the levator aponeurosis is lower, frequently as low as the superior tarsal border. This position allows the preaponeurotic fat pads to be present at a lower point on the upper eyelid, giving it a fuller appearance, and is found conjointly with a lack of attachment of the terminal strands of the levator aponeurosis from attaching to the subdermal surface of the pretarsal upper eyelid skin. The result is an apparently puffier ‘single eyelid’ without a crease (Fig. 9-3A).
In terms of fat distribution and compartments, Uchida2 first described the presence of four areas of fat pads in Asian eyelids:
Face
Onizuka and Iwanami3 note that Asians, particularly the Japanese, have a flat face and a head shape that is mesocephalic. The eyes tend not to be recessed deep in the orbit. These authors also find the lateral canthus to be 10 degrees superior to the medial canthus. They believe that creating an upper eyelid crease and removing any upper lid hooding would make the palpebral fissure appear wider and more open, which is aesthetically pleasing. I do not believe that all Asians have a lateral canthus 10 degrees above the medial canthus; however, certainly some of the other observations by these authors may be true.
Eyelid crease
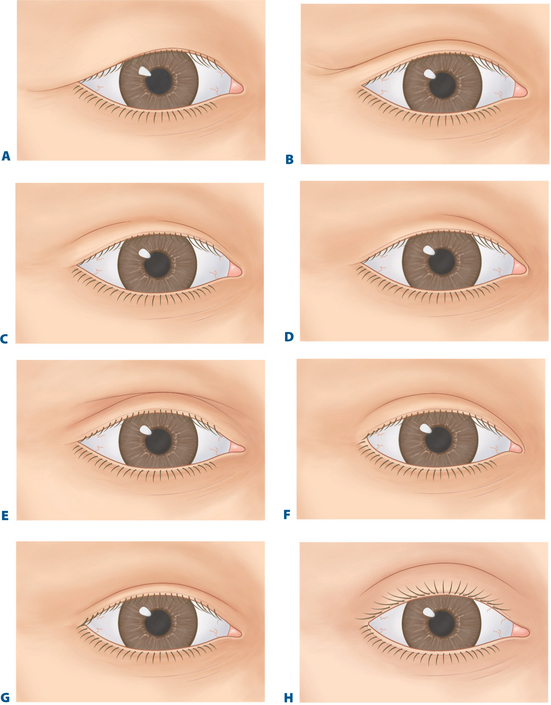
The configuration of the crease in the upper eyelids of Asians varies greatly. As I describe in other publications,4–6 the crease may be absent in one eye (see Fig. 9-3A) and present in the other. It may be continuous (see Fig. 9-3B) or discontinuous (see Fig. 9-3C). The crease may be partial or incomplete (usually present from the medial canthal angle and then fading laterally) (see Fig. 9-3D), and there may be multiple creases on an eyelid (see Fig. 9-3E).
Individuals who have a continuously formed eyelid crease may have either the inside-fold (nasal tapering) type of crease (see Fig. 9-3F) or a crease that is more parallel to the ciliary margin from the medial canthus to the lateral canthus (see Fig. 9-3G). With the inside-fold type, the crease may start from the medial canthal angle and gently flare away from the eyelid margin as it reaches the lateral canthal region (lateral flare) (see Fig. 9-3F
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Brow Lift Techniques
Brow Lift Techniques
 Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


