CHAPTER 22 Eyelid and Facial Laser Skin Resurfacing
Skin rejuvenation has long been a goal of medical practitioners. Time-honored remedies have included a wide range of chemical and mechanical agents, but the results were often much ado about little improvement, which might also be an apt description for many modern efforts! Perhaps the major difference between current practitioners and their predecessors is an understanding, albeit an imperfect one, of the treatment goals and of the methods to achieve them. The epidermis is tightly bound to the papillary dermis with an intervening basement membrane. The papillary dermis is about equal thickness to the epidermis and it blends into the much thicker reticular dermis. In a simplified understanding of skin anatomy, the appearance of the skin is largely a product of the regularity, or lack thereof, of the external layers of the skin.
Of special interest for facial skin anatomy is the presence of generous numbers of appendages which include hair follicles, sebaceous glands, and sweat glands. These structures arise within the deeper reticular dermis and subdermis. They each are connected to the skin surface by duct like structures which are lined with epithelium. During ablative resurfacing, the surface epithelium is completely removed. The epithelium from these glands provides the reservoir from which much of the re-epithelialization occurs. In contrast, the neck and especially the anterior chest wall have a paucity of these structures. This skin is a poor choice for resurfacing because the healing process is slow and prone to scarring. The goal of resurfacing is to induce significant improvement in the surface appearance of the skin. Alteration of the collagen in the papillary and upper reticular dermis is the method to achieve the goal. Before the advent of lasers, those changes were produced by a variety of topically applied chemical agents or by mechanical appliances such as dermabraiders. The expectation for both modalities was reformation of the papillary and upper reticular dermis with new, tightly cross linked, collagen bundles followed by re-epithelialization. By the late 1980s and early 1990s, carbon dioxide (CO2) laser vaporization was added to these modalities. Erbium laser vaporization was available by the mid 1990s. Both the CO2 and the erbium lasers ablate or remove the epidermis and the papillary and upper reticular dermis with precision and predictability. Their successful use requires an understanding of lasers, skin anatomy, and laser tissue interaction. Common to all ablative modalities including chemical peels, dermabrasion and laser ablation is production of a partial thickness wound in the skin which requires a ‘down time’ to heal. By the late 1990s another group of lasers, light sources and radiofrequency devices were introduced with the goal of inducing change in the collagen of the papillary and reticular dermis without damaging the epidermis. This group can collectively be grouped together as non-ablative devices. The number of wavelengths in this group and the variable parameters used to induce collagen neogenesis offer mute testimony to the fact that this technology is still developmental.
Laser physics
If the beam is released in a pulse with the intent to conduct it to the target without significantly modifying its physical characteristics, the power of the laser must be high enough to produce an appropriate effect when it reaches the target. Once this emitted laser light strikes tissue, it can be reflected, scattered, absorbed or transmitted. While reflection is not a very useful property in medicine, there are some applications where scattering can be employed to achieve therapeutic goals. The most useful current medical applications are absorption and transmission.
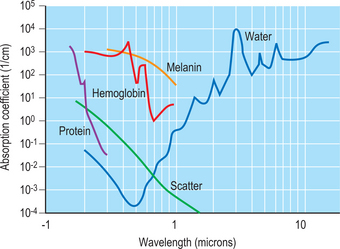
Our current concept of what happens when laser light and tissue interact was articulated by Anderson and Parrish1 in 1984 in their landmark paper describing selective photothermolysis. Specific components in tissue absorb light more intensely at some wavelengths than at others. These components are known as chromophores. For example, absorption by water peaks at 2900 nm and at 10600 nm. The erbium laser emits at 2940 nm and the carbon dioxide laser emits at 10600 nm. The incident energy from both of these lasers is rapidly absorbed by water in the most superficial layers of skin where it is converted to thermal energy. If the laser energy is sufficiently high, it will vaporize the water and in doing so will thereby remove or ablate the tissue. By controlling the incident energy and the duration of application, precise amounts of skin can be removed with limited collateral thermal damage.
Another example of this concept of absorption can be seen in the choice of an argon laser emitting at 514 nm (in the green part of the visible spectrum) where water absorption is very low and melanin absorption is relatively high. Energy emitted from this laser passes through the fluid medium of the eye to be absorbed by the chromophore melanin in the retinal pigment epithelium. The thermal energy generated by this effort can be useful in treating some pathology such as diabetic retinopathy. Figure 22-1 shows the different chromophores and their wavelengths of absorption. The goal of laser skin resurfacing is to vaporize or ablate surface tissue while minimizing thermal damage adjacent to the site of application. The obvious first step is to build the laser with enough power to reach the heat of vaporization, which in the case of water is 100°C. How efficiently this process of vaporizing tissue proceeds will be determined largely by the shape of the laser beam and the time of application. Since most medical lasers emit in either a true Gaussian shape or something similar to it, the most useful bell-shaped configuration will have the energy of the beam highly concentrated in the central portion of the beam. The objective in ablative resurfacing lasers is to exceed the energy of vaporization for the broadest area of the beam possible and to minimize the undesirable formation of thermally devitalized but intact skin on the margins of the beam. In prosaic terms, a beam configuration that looks more like a ‘high top hat’ than a ‘beret’ is desirable.
Duration of application of the laser beam can be a confusing parameter to understand. Conduction of any energy away from the site of origin/application requires time. When the water in tissue is the chromophore or target in tissue, the light energy is converted to thermal energy. If the laser energy is applied for a short enough time, thermal energy will be largely dissipated at the site. However if the energy is applied long enough, then the thermal energy will be conducted to the adjacent tissues. If this phenomenon occurs over a long enough time, significant thermal devitalization of the surrounding tissue is possible.2 Thermal burns can be produced that can dramatically alter the healing process, to the extent of scarring. This period of time before significant conduction occurs is defined as the thermal relaxation time of tissue. For skin, that time is about 400 microseconds (400 μsec). The challenge is to build a laser with enough power to treat a fairly large area of skin with a ‘short burst.’
An alternative to a single pulse is a scanner that will trace a small focused beam over the target rapidly enough to produce a desirable effect and still not expose the target area for longer than the thermal relaxation time of the tissue. Of course at the sides and depths of the beam, some subablative energy will exist which will produce a residual of thermally devitalized tissue beyond the area of application. Actually, this thermal residual can be helpful because it produces cauterization of small vessels which otherwise might bleed thereby obscuring the field.3 The effect of ablative laser applications can be predicted. The common denominator, at least among lasers of the same wavelength, is fluence which is the amount of energy applied per unit area. Fluence is measured in joules/cm2.
Laser safety
Laser safety is a requirement for all physicians. There are many regulatory levels in laser medicine: federal, state, local, departmental, and institutional. Before offering laser resurfacing or using any laser tool in practice, be sure to check with each level for safety standards. Federal regulations are outlined by the Occupational Safety Health & Administration (OSHA, www.osha.gov) in the form of general industry standards, directives, and compliance letters. Laser safety standards are specifically further delineated by the American National Standards Institute (ANSI). ANSI Z136.1-2000 document covers the general safe use of lasers. ANSI Z136.3-1996 document provides standards for the safe use of lasers in health care facilities. This document is most often used by regulatory groups and in litigation. Most states also maintain regulations as adjuncts to OSHA and ANSI standards, which may be even more rigorous.
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
Treatment of Lower Eyelid Dermatochalasis, Herniated Orbital Fat, and Hypertrophic Orbicularis Muscle
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


