CHAPTER 10 Upper Blepharoplasty Combined with Levator Aponeurosis Repair*
Defects or stretching of the levator aponeurosis are the most common causes of blepharoptosis seen in patients seeking cosmetic eyelid surgery. Upper eyelid blepharoplasty lends itself well to simultaneous correction of blepharoptosis via repair of aponeurotic defects. Blepharoplasty without correction of a preexisting blepharoptosis may aggravate the blepharoptosis. There are several advantages to the use of a combined procedure:
John R. Burroughs, William M. McLeish and Richard L. Anderson
Evaluation
The preoperative examination entails a thorough review of the physical relationships of the patient’s entire upper face. The heights and contours of the upper eyelids are noted with the forehead and eyebrows in a relaxed, natural position. An asymmetric or heavily furrowed brow often masks the presence of ptosis. Frequently, redundant upper eyelid skin must be gently elevated out of the way to visualize the lid margin and the natural eyelid crease, which is typically elevated by an aponeurosis disinsertion.
Surgical technique
The skin incision is marked superiorly to circumscribe redundant skin and orbicularis muscle tissue. The surgeon establishes the proper amount of skin and muscle that can be safely excised by placing one blade of a smooth forceps on the marked eyelid crease incision and gently pinching sufficient redundant tissue between it and the second blade of the forceps to cause the lid margin to just begin to evert. We use the extra fine point skin marker by ScanlanTM (800-328-9458) as it has an ultra fine tip and allows precise marking. This maneuver is repeated along the length of the eyelid crease incision, and the superior extent of the incision is marked with a pen at each location (Fig. 10-1A). As a general guide, the superior limb of the incision should be at least 10–12 mm below the inferior margin of the eyebrow at the midpupillary position to ensure adequate anterior lamella remains to allow for complete eyelid closure and to prevent iatrogenic brow ptosis.
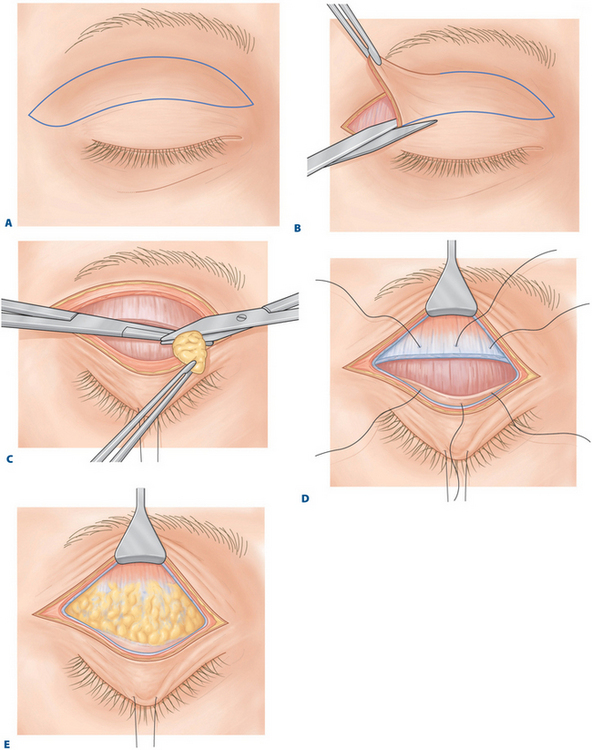
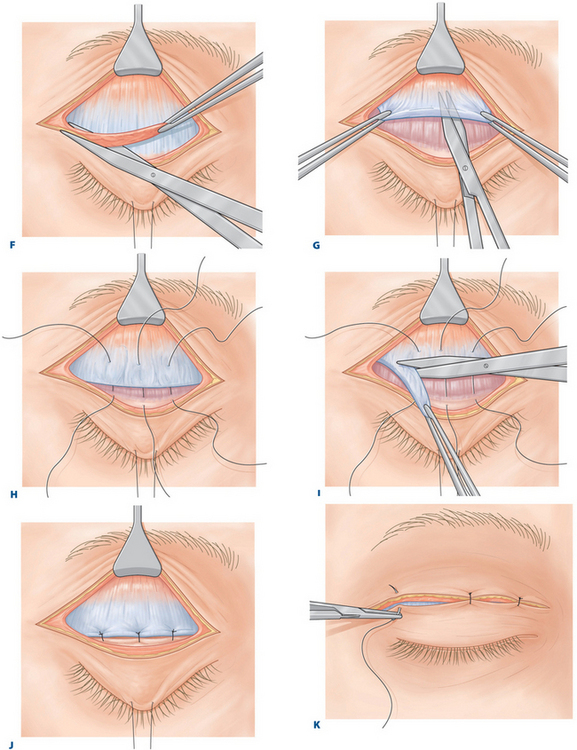
Figure 10-1 A, Ellipse of upper eyelid skin to be removed is outlined.
E, Alternative 2: Fatty infiltration of the levator aponeurosis. No distinct disinsertion is noted.
I, Alternative 2: The redundant levator aponeurosis is excised.
J, The 5-0 polyglactin sutures are secured.
Related posts:
 Chemical Peeling: Independent or in Conjunction with Facial Plastic Surgery
Chemical Peeling: Independent or in Conjunction with Facial Plastic Surgery
 Brow Lift Techniques
Brow Lift Techniques
 Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


