The Clinical Problem ( Fig. 36.1 )
Synopsis
Performing procedures to rejuvenate the arm requires an understanding of the aesthetic arm deformity and its pathophysiology. Excisional techniques (e.g., brachioplasty), liposuction, and nonsurgical treatment options may all be used for arm rejuvenation. There are a number of technical points that can make brachioplasty a reliable and rewarding procedure.

The Aesthetic Problem
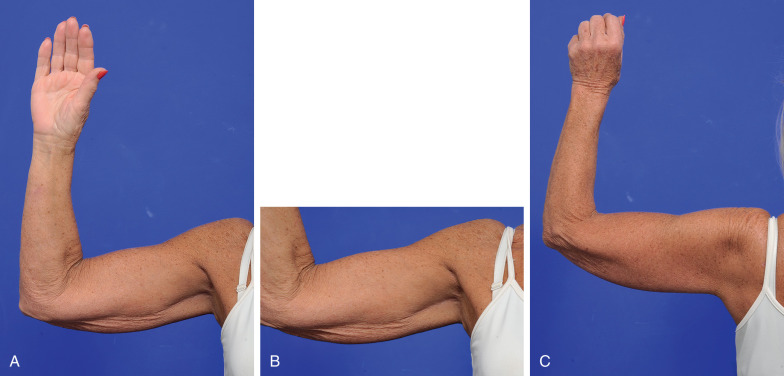
This 67-year-old woman (see Fig. 36.1 ) was unhappy with the presence of loose skin hanging from her arms. She didn’t think that her arms were harmonious with her overall appearance and was reluctant to wear short-sleeve tops or dresses.
Two categories of patients present for rejuvenation of the arm:
- 1.
The patient with signs of aging
- 2.
The massive weight loss patient
These patients present with the following signs:
- •
Redundant skin, with or without excess soft tissue
This produces increased wrinkling and folds and is most pronounced in the inner (posteromedial) aspect of the arm. Pascal and Le Louarn have described this excess skin as analogous to a sleeve that is too wide and too long.
- •
Increase in the inferior curve of the arm
This is seen when the arm is abducted to 90 degrees at the shoulder, the so-called bat wing or bingo wing deformity. It occurs with aging and was quantified by Glanz and Gonzalez-Ulloa using the coefficient of Hoyer. This ratio of the relative height of the soft tissues above and below the inferior border of the humerus increases from 1 : 1 to 1 : 2.2 between the ages of 10 and 70 years.
- •
Loss of axillary hollow
- •
Lipodystrophy
General Considerations
- 1.
Skin quality—thickness, extent of solar damage, senile changes
- 2.
Excess skin—quantity and distribution
- 3.
Excess fat—quantity and distribution
In Case 36.1 (see below), the patient had poor skin quality. It was thin and had significant solar damage (see Fig. 36.1E ). She had a moderate excess of skin involving the entire arm with loss of the axillary hollow and had minimal excess fat. The desired outcome in this situation was to narrow and shorten the sleeve of the arm with concomitant deepening of the axillary hollow.
Surgical Preparation and Technique
Management and Treatment Options ( Table 36.1 )
Nonsurgical Treatment Options
There are an increasing number of transcutaneous energy delivery devices currently available. Broadly speaking, they are classified according to the type of energy they deliver to their target—mechanical (e.g., suction, massage), radiofrequency, ultrasound, cryolipolysis, and laser. Of these, radiofrequency devices are the most popular.
| FAT EXCESS | |||
|---|---|---|---|
| SKIN EXCESS | Minimal | Moderate | |
| Minimal | Non-surgical treatment options Axillary vertical excision Short-scar arm reduction | Circumferential liposuction +/− Axillary or short-scar reduction | |
| Moderate | Standard brachioplasty +/− Lateral chest wall extension | Circumferential liposuction +/− Standard brachioplasty +/− Lateral chest wall extension | |
Adverse outcomes following noninvasive body-contouring treatments are uncommon but may include thermal injuries and temporary dysesthesia.
Liposuction
Liposuction can be used alone, in select patients, to provide satisfactory reduction in arm circumference with some associated skin retraction. It has also been established that it is safe to perform brachioplasty in conjunction with liposuction outside the region of excision. With regard to the latter, we advocate using the principles of SAFE (separation, aspiration, and fat equalization) liposuction.
Excisional Techniques
In the massive weight loss patient, the skin excision may need to be extended onto the chest (lateral chest wall extension; Fig. 36.2 ).
Case 36.1
This patient had a problem of excess skin of the whole arm, with minimal excess fat. Liposuction alone was considered unlikely to be effective in achieving an improvement in contour and satisfactory skin contraction. She understood the necessity for an excisional procedure but was unwilling to accept a long scar. Thus, the options for a modified brachioplasty and its inherent limitations were discussed.
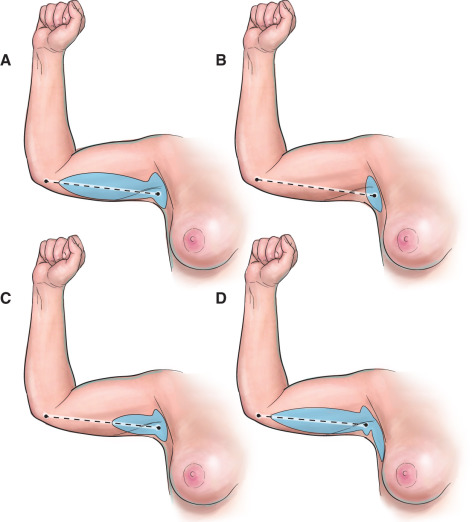
Under general anesthesia, she underwent a bilateral short-scar arm reduction with axillary suspension. The vertical limb measured 6 cm and was located in the axilla. The horizontal limb was 6.5-cm long and located in a posteromedial position. Axillary suspension using two 3-0 Prolene sutures secured the superficial fascial system (SFS) of the posteromedial arm to the axillary fascia. The remaining SFS was then closed with 3-0 Vicryl and the subcuticular layer with 4-0 V-Loc sutures.
It was clear within 6 months postoperatively that although the appearance of her arms was much improved and her scars were satisfactory, there was residual skin excess of the distal arm to elbow ( Fig. 36.3 ).The patient agreed to an extension of her scar and underwent revision to a bilateral standard arm reduction.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


