Upper Arm Lift (Brachioplasty)
Jennifer Capla
Joseph Michaels
DEFINITION
A brachioplasty or upper arm lift is a procedure that targets the skin excess from the axilla to the elbow.
The “hammock”-like effect of loose skin is sometimes known as “bat wings.”
ANATOMY
With the arm abducted and flexed at 90 degrees, the important landmarks for assessment are from the apex of the axillary crease to the olecranon (FIG 1).
The bicipital groove is the area between the biceps brachii above and the long head of the triceps below.
In the bicipital groove, below the brachial fascia, lie several important neurovasculature structures including the median and ulnar nerves and the axillary artery and vein.
In the midportion of the upper arm over the bicipital groove, superficial to the brachial fascia, lies the medial brachial cutaneous nerve.
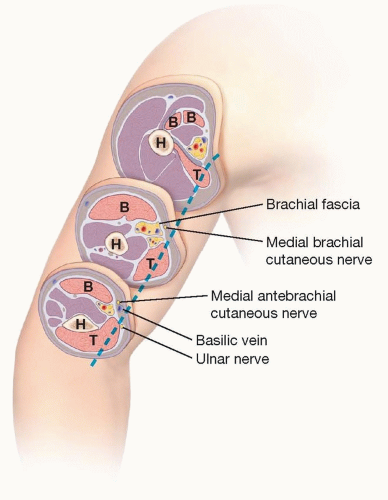
FIG 1 • Arm serial sections over bicipital groove. The blue dotted line approximates scar position in the bicipital groove. B, biceps tendon; T, triceps muscle; H, humerus.
In the distal portion of the upper arm over the bicipital groove, superficial to the brachial fascia, lies the medial antebrachial cutaneous nerve and the basilic vein.
PATHOGENESIS
Factors that can produce laxity of the upper arm soft tissue:
Significant weight changes
Aging
Previous liposuction
Sun damage
Despite a good exercise regimen, skin may not retract. This is likely due to weakness of the connections of the superficial fascial system to the axillary fascia.
PATIENT HISTORY AND PHYSICAL FINDINGS
A history of significant weight loss, aging, or previous liposuction can lead to skin excess of the upper arms.
Patients complain of loose hanging skin of the upper arms that interferes with daily activities, difficulty with finding shirts that fit, and the need to wear long sleeves even in the summer to cover up due to embarrassment of the tissue excess.
Physical examination:
Examine the patient with arms abducted at 90 degrees and the forearm flexed at 90 degrees.
Visible skin excess from the axilla to the elbow that drapes like a hammock.
Determine residual adiposity vs skin laxity.
Assess for any arm swelling or lymphedema.
Contraindications: chronic swelling from lymphedema or venous incompetence
IMAGING
No radiologic imaging or diagnostic testing is necessary.
SURGICAL MANAGEMENT
Preoperative Planning
Assess the patient’s goals—in front of the mirror with the arm abducted and flexed at 90 degrees, use the pinch technique to demonstrate what the arm lift will achieve.
If the patient has significant residual adiposity, an arm lift alone may leave the patient with a heavy arm. Consider liposuction prior to debulk the arm, and then return for an arm lift at a second stage. If the majority of fat is in the posterior compartment of the arm, then liposuction can be combined with the procedure.
Weight loss patients should be weight stable for a minimum of 3 months. Nutritional assessment is an important factor in wound healing. Labs should include albumin, prealbumin, TIBC, and folate.
Managing expectations: Preoperative discussion with the patient about the scar ensures that the patient understands the trade-off. Brachioplasty scars can be red, raised, thickened, and cordlike. Take a black sharpie and mark the approximate position of the scar on the patient. This allows them time to go home and look in the mirror to make sure that they are willing to trade for the scar.
Scar position: The brachioplasty scar can be positioned in either the bicipital groove or the posterior arm. A patient should be given the opportunity to choose. We prefer the bicipital groove for scar location. There are patients in certain professions, like teachers, who raise their arms a great deal and have opted for the posterior scar.
Bicipital groove scar—visible from the front view when the arm is abducted and flexed, but when the arm is down at the patient’s side, it is not seen.
Posterior scar—not visible from the front or back when the arm is abducted and flexed, but when the arm is down at the patient’s side, it can be seen from behind.
Marking the patient preoperatively is of utmost importance.
Using the pinch technique, a guide to the excision pattern can be determined. Pay careful attention to the pull in the axilla and the lateral chest wall to ensure that there is no distortion on the chest/breast area.
If any arm bands are present, then resection may lead to worsening of the bands (“Popeye deformity”) that you must make the patient aware of before surgery.
Speak with your anesthesiologist:
IV placement in the hand, not the antecubital fossa
Blood pressure cuff on the leg or forearm
If performing more than one procedure, it is best to start with the arms. If not, discuss with the anesthesiologist about the possibility of limiting IV fluid to decrease overall swelling until the arm resections are performed.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








